
 Download:
Download:




-
In Guangdong Province, children under 2 years old are commonly given 10 types of National Immunization Program (NIP)-recommended vaccines (BCG, HepB, IPV, bOPV, DTaP, MPV-A, MR, JE-L, HepA-L, MMR) given in 17 doses and 6 non-NIP vaccines (Rotavirus, PCV13, Hib, EV71, Influenza, and Chicken Pox) given in 16 doses (1-2). Then Guangdong issued the vaccination abnormal response compensation insurance and Co-Administration of Multiple Vaccines policy (3-4). Previously, to administer these 33 vaccine doses, 25 visits to the vaccination clinic were required, but the policy has theoretically reduced the number of required visits to 14 (1,5). This study used children under 2 years old registered in the National Immunization Program Information Management System (NIPIMS) as the sampling population, and survey participants were selected by stratified random sampling. Relevant data were collected through interviews conducted in-person or by telephone, and costs due to transportation and work absences to receive these vaccinations were estimated for the children’s families. A total of 591 children’s parents were interviewed, and the average costs were estimated at 103.42 RMB per clinic visit. This policy could save about 1137.62 RMB for each child during their first 2 years of life. To provide scope, 1.8 million infants in Guangdong received the first dose of Hepatitis B vaccine in 2018; based on the number of children, this policy could therefore save up to 2.0 billion RMB for families in Guangdong Province for this single vaccination event. The Co-Administration of Multiple Vaccines Policy can significantly reduce vaccination costs for children’s families and can greatly improve the social cost-effectiveness of childhood vaccinations. Our findings suggest that Co-Administration of Multiple Vaccines should be implemented as soon as possible.
This study estimated the cost incurred by the families with children under 2 years old in Guangdong Province during the process of inoculation. Children were randomly selected from NIPIMS, and duplicate cases and cases without phone numbers were excluded. In Guangzhou and Shenzhen, relevant phone numbers could not be collected so children’s families were interviewed in-person. The cost of transportation included the fee of taking public traffic (subway, bus, or taxi) or by calculating unit distance or unit time (driving cars, motorcycles, or battery cars) (6–8). Work absences were measured as the time required for all the accompanying personnel to complete the whole inoculation process. The data was inputted by double-entry using Epidata3.1 and then organized into a database with Excel 2016, and descriptive statistical analysis was performed with SPSS 21.0.
A total of 1,720 calls were made, 635 persons answered the phone (response-rate 36.92%), and 430 persons were effectively interviewed (effective-response-rate 67.72%). An additional 219 persons were interviewed in-person (response-rate 100%), and 161 persons were effectively interviewed (effective-response-rate 73.52%). Ultimately, 591 children’s families were included in the final sample (Table 1).
Region Number of
interviews (%)Accompanied
personsClinic distance *
(km)Work absence
time *
(Hour)Transportation
time †
(Hour)Total time per
clinic visit *
(Hour)1 2 >2 Pearl River Delta 351(59.39) 117 215 19 2.00(1.00, 4.00) 2.00(1.00, 3.00) 0.44(0.41, 0.47) 1.65(1.57, 1.74) East Guangdong 80(13.54) 18 59 3 3.30(2.00, 8.50) 1.00(1.00, 2.00) 0.44(0.38, 0.49) 1.33(1.18, 1.49) West Guangdong 85(14.38) 27 54 4 4.25(2.00, 5.15) 2.00(1.50, 3.00) 0.50(0.43, 0.57) 1.50(1.33, 1.66) North Guangdong 75(12.69) 38 37 0 3.00(1.28, 6.00) 1.50(1.50, 2.00) 0.38(0.33, 0.43) 1.24(1.07, 1.41) Guangdong 591(100) 200 365 26 2.00(1.00, 5.00) 2.00(1.00, 3.00) 0.44(0.41, 0.46) 1.54(1.47, 1.60) * The data presented a non-normal distribution and was represented by median and quartile (P25, P75).
† The data was normally distributed and expressed as a mean and 95% Confidence Interval.Table 1. The aspects of vaccination clinic visits in Guangdong Province
The median total cost was 103.42 RMB per clinic visit, the median transportation cost was 5.20 RMB per clinic visit, and the median work-absence cost was 93.42 RMB per clinic visit. The region with the highest total cost per clinic visit was the Pearl River Delta, the median total cost was 148.56 RMB per clinic visit (Table 2).
Region Hourly wage per capita (RMB) Transportation cost per clinic visit * (RMB) Work absence cost per clinic visit * (RMB) Total cost per clinic visit * (RMB) Pearl River Delta 62.28 4.00(0.00, 16.00) 124.56(41.30, 186.84) 148.56(124.56, 253.12) East Guangdong 17.92 10.00(4.00, 20.00) 35.85(26.88, 53.76) 52.30(35.84, 73.76) West Guangdong 21.96 2.80(0.40, 11.00) 43.92(21.96, 76.86) 52.92(37.11, 88.64) North Guangdong 16.52 4.00(0.00, 10.00) 24.78(16.52, 33.04) 33.04(20.52, 46.52) Guangdong 39.59 5.20(0.00, 16.00) 93.42(41.30, 186.84) 103.42(50.78, 186.84) * The data presented a non-normal distribution and was represented by median and quartile (P25, P75). Table 2. The costs of vaccination clinic visits in Guangdong Province
Before the Co-Administration of Multiple Vaccines Policy, vaccines in different category could not be co-administered. As a result, children under 2 years in Guangdong Province required 25 visits to the vaccination clinic to complete the 33 required doses of 16 types of vaccines. After implementing the Co-Administration of Multiple Vaccines Policy, the number of required clinic visits has potential to be reduced from 25 visits to 14 visits. But there were some vaccines (DTaP-IPV/Hib, DTaP/Hib, PCV13, Bivalent HPV and Tetravalent HPV) that could not be recommended to be co-administered under Chinese vaccine instructions. (Figure 1)
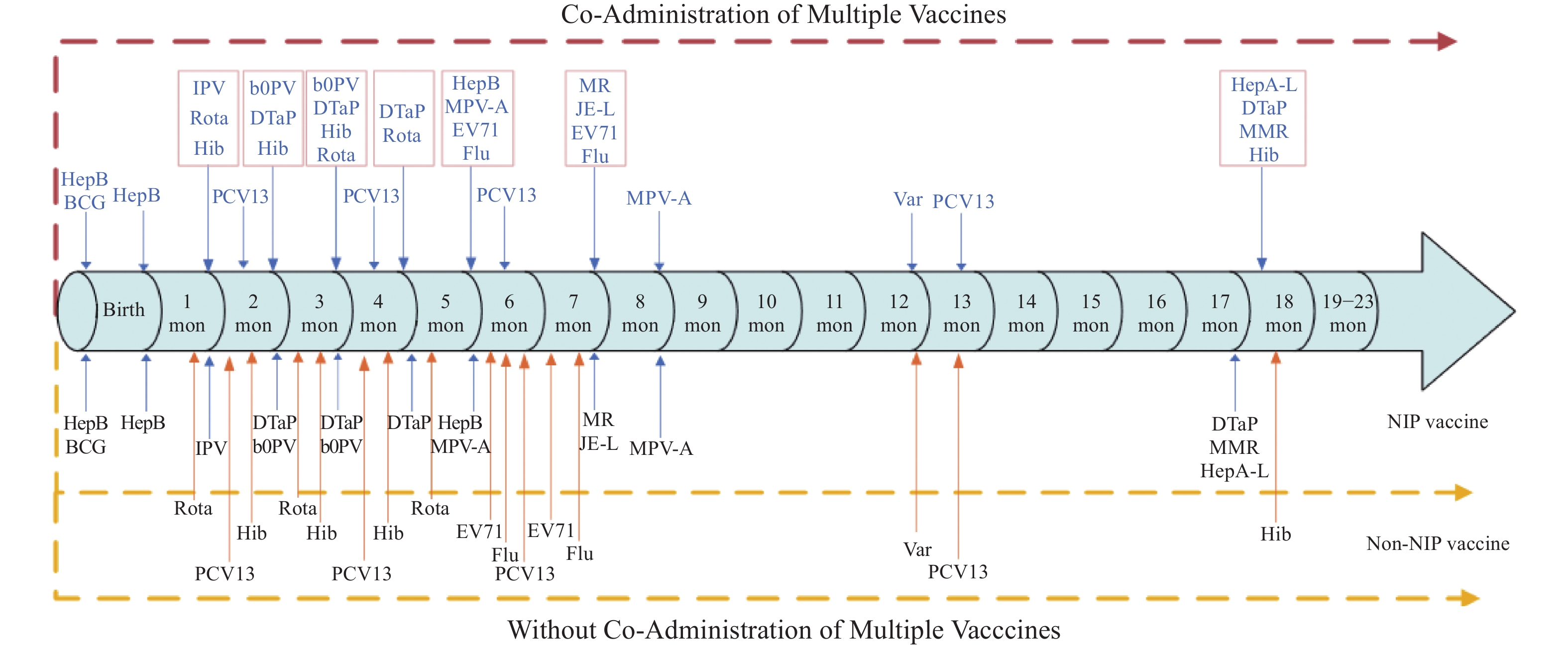 Figure 1.
Figure 1.Comparison of inoculation schedule before and after the Co-Administration of Multiple Vaccines Policy
Note: PCV13 cannot be administered with other vaccines because of the Chinese vaccine instruction. Abbreviation: BCG: Bacillus Calmette – Guerin Vaccine; Hep-B: Hepatitis B Vaccine; IPV: Inactivated Poliovirus Vaccine; b-OPV: Bivalent Oral Poliomyelitis Vaccine; DTaP: Diphtheria Tetanus Pertussis Vaccine; MPV-A: Meningococcal Poly-saccharide Vaccine, A; MR: Mumps and Rubella Vaccine; JE-L: Japanese Encephalitis Vaccine, Live; HepA-L: Hepatitis A Vaccine, Live; MMR: Measles, Mumps and Rubella Vaccine; PCV13: Pneumococcal Polysaccharide Conjugate Vaccine, 13-valent; Hib: Haemophilus influenzae type B Vaccine; EV71: Enterovirus 71 Inactivated Vaccine.
HTML
-
Previous research on vaccines focuses more on the cost of production, storage, and transportation as well as the valuation of vaccine effectiveness. However, fewer studies evaluate the cost to families associated with visiting the clinic in terms of transportation and absences from work that exclude the cost of vaccines.
In the past, NIP vaccines and non-NIP vaccines generally could not be co-administered because of the different funding sources for compensation insurance for routine immunization. In 2018, Guangdong Province issued adverse events compensation insurance for routine immunization. The insurance cost is jointly shared by the government and by the vaccine enterprises. The basic insurance costs of NIP vaccines are paid using the special fund for the development of health and family planning. The basic insurance costs of non-NIP vaccines are paid by vaccine enterprises. Insurance companies will pay for all abnormal reactions following vaccination (3).
The amount in savings (2.2 billion RMB) for families in Guangdong Province as a result of the Co-Administration of Multiple Vaccines Policy was a theoretical maximum savings as it was not based upon the actual uptake of non-NIP vaccines. The actual savings will depend on how many families use non-NIP vaccines that are co-Administered with NIP vaccines. We found that savings in the Pearl River Delta (1.9 billion RMB) far exceeded other regions (0.3 billion RMB). This may be due to the larger number of people accompany the children, the longer work-absences, and the higher level of per-capita wages in the Pearl River Delta.
This study is subject to at least four limitations. First, the telephone interviews might be subject to recall bias, and in-person interviews may be subject to selection bias. Second, using both telephone interviews and in-person interviews might affect the consistency of the data (9-10). Third, there is no comparison between urban and rural areas, which may include relatively large disparities in results. Fourth, this study did not account for differences in the willingness of people in different regions to consume non-NIP vaccines.
Future research could evaluate the precision of vaccine co-administration, whether the NIP vaccines could be administered on schedule, and if this policy could increase coverage for non-NIP vaccines. To reduce the number of vaccination clinic visits required for children, more research should be done on co-administration of vaccines and on combining vaccinations.
| Citation: |

|