

 Download:
Download:




-
China has achieved commendable success in stabilizing human immunodeficiency virus (HIV) prevalence at a relatively low level of transmission (1). Nevertheless, the total number of people living with HIV in China rose to approximately 1.05 million, with cumulative reported acquired immune deficiency syndrome (AIDS)-related fatalities reaching 351,000 by the end of 2020 (2). Since the initial infiltration of HIV into China in 1982 (3), the nation has enacted over 471 national policies through 2021 to combat the epidemic. Initially, the outbreak was perceived primarily as a healthcare issue rather than the complex societal challenge that it manifested into. The Ministry of Health (MOH, now known as National Health Commission) was initially tasked with HIV prevention, issuing the nation’s first HIV/AIDS-related policy in 1984, which aimed to ban HIV-infected products and individuals from entry. Regrettably, this approach proved inadequate as significant HIV outbreaks unfolded. At this juncture, the State Council Research Office recognized the HIV epidemic as a grave societal and public health issue, posing a threat to the “Survival of the Chinese Nation” (4). Engagement at a higher governmental level became imperative to coordinate an effective response across diverse administrative agencies.
In 1995, the State Council issued “the Notice on Strengthening the Prevention and Control of AIDS (NSPCA)”, creating the first policy specifically dedicated to orchestrating a cohesive HIV response among government agencies. The following year, the State Council advanced this effort by approving the establishment of the Issues Concerning the Coordination Conference System for the Prevention and Control of AIDS and Sexually Transmitted Diseases (STDs). This system introduced a formal coordination mechanism that encompassed various agencies (5). By 2004, in an effort to further enhance the leadership and collaboration in the fight against HIV/AIDS, the State Council formally established the State Council AIDS Working Committee (SCAWC).
China’s evolving approach to HIV/AIDS policy has been the subject of extensive scholarly attention, encompassing reviews of institutional changes (6), specific policy shifts (7), and the history of the HIV epidemic within the country (8). Studies to date have discerned a correlation between the epidemiology of HIV/AIDS and policy responses. Despite previous efforts, most analyses have focused on a limited selection of key policies, with the exception of Yan et al.’s comprehensive examination of national-level HIV/AIDS policies, which cataloged 217 policies implemented from 1984 to 2005 (9). However, even this thorough study did not investigate the relationship between policy development and the various governmental bodies responsible for them. Moreover, in the two decades since that study, there has been substantial progress.
To date, insufficient attention has been devoted to the examination of HIV/AIDS policies. Research indicates that the delivery of healthcare policies necessitates considerable collaboration; a deficiency in coordination frameworks may constitute a significant barrier to the provision of integrated services (10-11). The establishment of a policy coordination mechanism is essential for the effective prevention of HIV/AIDS transmission. How this coordination mechanism is structured and the nature of its formation are questions that remain unanswered. This article seeks to enrich the theoretical discourse on the evolution of China’s HIV/AIDS policy by scrutinizing the interconnection between policy development and coordination mechanisms.
-
Our data acquisition encompassed a wide array of materials linked to HIV/AIDS spanning from 1982 to 2021. This collection comprises national policy documents, detailed accounts of significant outbreaks, and expressive commentary from esteemed entities such as high-level government dignitaries, delegates of the National People’s Congress (NPC), and members of the Chinese People’s Political Consultative Conference (CPPCC). Additionally, we included insights from public health authorities, HIV/AIDS activists, and other influential individuals who have made significant contributions to combating HIV/AIDS. The data collection process for this study involved sourcing material from a variety of reputable online platforms and scientific journal publications (12-15)
1 . By the conclusion of the data collection in February 2022, a comprehensive set of 471 relevant documents issued by China’s central government from 1982 to 2021 had been amassed. -
Drawing upon the contents of the text and consultations with experts, we examined the trajectory of policy evolution across three dimensions: the substance of the policies, the stakeholders involved, and the governmental levels at which the policies were enacted. To quantify this analysis, we devised a set of indicators organized into three categories: policy focus areas; government agencies responsible for issuing policies; and the scope of government agendas.
Identification and Categorization of Policy Focus Areas: We endeavor to refine the methodology for classifying policies according to their salient content. Upon reviewing the content, we categorized 471 pertinent policies and events into 16 distinct classifications, as delineated in Table 1.
Policy indicators Variables Policy focus areas 1) Treatment
2) Public education
3) Surveillance and monitoring
4) Social engagement and participation
5) Governmental departments coordination
6) Oversight and evaluation of policy implementation
7) Assistance to people affected by HIV/AIDS
8) Strategic plans
9) International collaborations
10) Specific interventions to transmission routes
11) Scientific studies and researches
12) Comprehensive policies
13) Initiations & reforms of government program management mechanism and personnel training
14) Academic conferences
15) Press releases
16) Other areasGovernment agencies which have issued policies 1) State Council and/or Central Party Committee (CPC)
2) Ministry of Health (MOH)
3) Other Ministries (Ministries or Agencies other than the MOH collaborated to issue policies together, without an apparent lead)
4) MOH-Led with Other Ministries (MOH led and other Ministries participated)
5) Other Ministry Led (Another Ministry/Agency led with participation from multiple ministries/agencies, MOH may also participate)Level of government agendas 1) DAP (1982–1994)
2) NAP (1995–2021)
a) a period of Jointly Conferences (1995–2003)
b) a period of SCAWC established (institutionalized) (2004–2021)Table 1. HIV/AIDS policy development indicators.
Policies promulgated by either individual or multiple governmental bodies: Certain policies have emanated from a solitary agency, whereas others have been collaboratively issued by multiple responsible entities. The count of agencies engaged acts as a barometer for gauging the level of priority attributed to HIV/AIDS policy measures.
Governmental response stratification: the evolution of China’s HIV/AIDS policy coordination mechanism has led to its classification into distinct phases: the initial Department-Agenda Period (DAP) (1982–1994), followed by the comprehensive National (State-Council)-Agenda Period (NAP) (1995–2021). The NAP bifurcates further into two stages: the earlier Joint Conference Period (1995–2003), designated as NAP I, and the subsequent SCAWC Period (2004–2021), hereafter referred to as NAP II.
-
We conducted an analysis to illustrate the evolution of HIV/AIDS policies from 1984 to 2021, presenting the changes in the form of a line chart. Additionally, a cross-tabulation analysis was performed to examine the relationship between policy indicators and the policy coordination mechanism.
-
Figure 1 shows changes in the number of HIV/AIDS policies from 1984 to 2021. The annual number of policies varied significantly, with a peak in 2004 at 36 policies. Notably, a consistently high number of policies were issued from 2005 to 2007. In 1995, another peak occurred with 29 policies. Before 1995, policy issuance was low, averaging 5.2 policies per year. The fewest policies were issued in 1984 and 1994. The periods between 1996–2003 and 2008–2021 saw relatively large and stable outputs of policies following the peak years. Since 2000, approximately 10 policies were issued annually (except in 2013), though the yearly maximum did not exceed 20 policies.
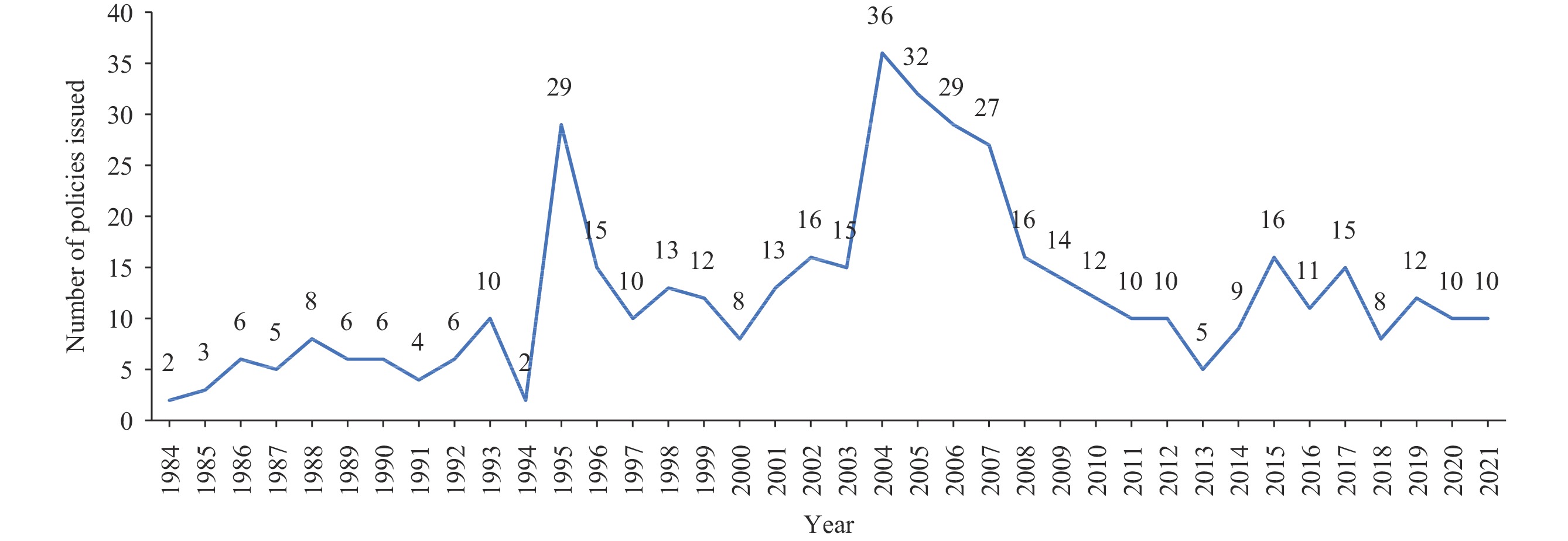 Figure 1.
Figure 1.Number of policies issued from 1984 to 2021.
-
Table 2 presents the responsible government agencies and policy focus areas. China has promulgated a total of 471 HIV/AIDS-related policies, of which 85 (18.0%) pertain to public education.
Policy focus areas n (%) Issuing agencies State Council
(n=104), %MOH
(n=223), %Other ministries*
(n=61), %MOH-led with other ministries
(n=50), %Other ministry led†
(n=33), %Treatment 28 (5.9) 1.0 8.5 6.6 2.0 9.1 Public education 85 (18.0) 21.2 11.2 23.0 24.0 36.4 Surveillance and monitoring 26 (5.5) 1.9 8.5 1.6 8.0 0.0 Social engagement and participation 6 (1.3) 0.0 0.9 0.0 6.0 3.0 Governmental departments coordination 25 (5.3) 14.4 3.6 3.3 0.0 0.0 Oversight and evaluation of policy implementation 23 (4.9) 7.7 5.4 1.6 4.0 0.0 Assistance to people affected by HIV/AIDS 8 (1.7) 0.0 0.4 6.6 2.0 6.1 Strategic plans 25 (5.3) 14.4 2.7 3.3 4.0 0.0 International collaborations 25 (5.3) 4.8 8.1 0.0 2.0 3.0 Specific interventions to transmission routes 66 (14.0) 1.9 20.6 8.2 22.0 6.1 Scientific studies and researches 35 (7.4) 1.0 4.0 24.6 10.0 15.2 Comprehensive policies 37 (7.9) 7.7 8.5 9.8 4.0 3.0 Initiations & reforms of government program management mechanism and personnel training 21 (4.5) 5.8 4.9 3.3 2.0 3.0 Academic conferences 9 (1.9) 0.0 2.7 0.0 2.0 6.1 Press releases 6 (1.3) 1.0 2.2 0.0 2.0 0.0 Other areas 46 (9.8) 17.3 7.6 8.2 6.0 9.1 Abbreviation: MOH=ministry of health; HIV=human immunodeficiency virus; AIDS=acquired immune deficiency syndrome.
* Other Ministries: ministries (other than the MOH) collaborated to issue policies together, without an apparent lead.
† Other Ministry Led: a ministry other than the MOH led the policy development, however, the MOH may still be part of the policy development.Table 2. Policy focus areas by issuing agencies.
In examining the distribution of policies promulgated by specific agencies since 1984, it is evident that the State Council issued 104 policies, the MOH issued 223, while other ministries issued 61. There were also collaborative efforts, with the MOH leading and supported by other ministries in issuing 50 policies, and other ministries leading in the issuance of 33 policies. Regarding the types of policies issued, public education was a predominant focus for the State Council, collaborative efforts led by the MOH, and initiatives led by other ministries, with respective emphasis of 21.2%, 24.0%, and 36.4%. The State Council concentrated more on coordinating government departments and implementing strategic plans, with each area receiving 14.4% of its policy efforts. The MOH, tasked with drafting health-related policies, emphasized specific interventions targeted at transmission routes (20.6%), as well as endorsing comprehensive policies, surveillance, and monitoring (each at 8.5%). Other ministries and ministry-led initiatives placed a significant emphasis on scientific studies and research with these categories receiving 24.6% and 15.2% of the policies, respectively. For the MOH-led collaborations with support from other ministries, the focus after public education was on specific interventions to address transmission routes, which accounted for 22.0% of the policies.
-
Table 3 presents the distribution of policies issued by agencies as well as by periods over the past four decades, demonstrating a significant shift in the perception of HIV/AIDS from an issue of MOH-level importance to one of national importance.
Items Whole period
(1982–2021)Level of government agendas DAP (1982–1994)
MOH agendaNAP (1995–2021) NAP (1995–2021) NAP I (1995–2003) NAP II (2004–2021) Total policies issued (n) 471 58 413 131 282 Average policies per year (n) 11.8 4.5 15.3 14.6 15.7 Government agencies issued policies (%) State Council 22.1 10.3 23.7 13.7 28.4 Ministry of Health 47.3 56.9 46.0 61.8 38.7 Other ministry 13.0 10.3 13.3 13.0 13.5 Health led with other ministries 10.6 19.0 9.4 9.2 9.6 Other ministry led 7.0 3.4 7.5 2.3 9.9 Policy focus areas (%) Treatment 5.9 1.7 6.5 6.9 6.4 Public education 18.0 12.1 18.9 13.7 21.3 Surveillance and monitoring 5.5 15.5 4.1 6.1 3.2 Social engagement and participation 1.3 3.4 1.0 0.0 1.4 Governmental departments coordination 5.3 1.7 5.8 9.9 3.9 Oversight and evaluation of policy implementation 4.9 1.7 5.3 3.1 6.4 Assistance to people affected by HIV/AIDS 1.7 0.0 1.9 0.0 2.8 Strategic plans 5.3 3.4 5.6 5.3 5.7 International collaborations 5.3 3.4 5.6 9.9 3.5 Specific interventions to transmission routes 14.0 24.1 12.6 19.8 9.2 Scientific studies and researches 7.4 3.4 8.0 2.3 10.6 Comprehensive policies 7.6 10.3 7.3 6.1 7.8 Initiations & reforms of government program management mechanism and personnel training 4.5 12.1 3.4 3.8 3.2 Academic conferences 1.9 0.0 2.2 4.6 1.1 Press releases 1.5 3.4 1.2 2.3 0.7 Other areas 9.8 3.4 10.7 6.1 12.8 Abbreviation: HIV=human immunodeficiency virus; AIDS=acquired immune deficiency syndrome; DPA=department-agenda period; MOH=ministry of health; NAP=national-agenda period; NAP I=Joint Conference Period; NAP II=State Council AIDS Working Committee Period. Table 3. HIV/AIDS policy development by government policy agenda periods.
The approach to policy coordination underwent significant evolution over the years. Initially, from 1982 to 1994, there was an absence of any formal coordination mechanism. This shifted in the period from 1995 to 2003, during which a coordination mechanism existed, albeit without the support of a formally established committee. Subsequent to this phase, a formal committee was established.
During the DAP era, governmental entities functioned autonomously, frequently with conflicting objectives, employing rigid regulatory instruments without harmonized collaboration or the institutional adaptability to adjust to evolving circumstances over time. Conversely, in the NAP phase, the approach to HIV/AIDS policy extended beyond the confines of the healthcare sector and treatment in isolation. The State Council shifted its emphasis to broader public education initiatives, the coordination of government departments, strategic planning, and additional sectors.
-
During the DAP, the MOH was responsible for formulating and promulgating over half of the policies, accounting for 56.9%.
In the analysis of the NAP (1995–2021), there is a discernible trend in the reallocation of policy-making authority. The MOH, whether acting independently or in collaboration with other ministries, experienced a reduction in its share of policy initiatives — from 56.9% to 46% for MOH-led policies, and from 19.0% to 9.4% for those involving a partnership with other ministries. In contrast, the role of the State Council in policy enactment has more than doubled, increasing from 10.3% to 23.7%.
During the NAP I (1995−2003), there was a discernible shift in the pattern of policy-making among governmental entities. The State Council saw its contribution to policy issuance rise from 10.3% to 13.7%. Nevertheless, the MOH retained a significant influence throughout this era, originating 61.8% of the policies and spearheading an additional 9.2% of policy development efforts. Consequently, the MOH was responsible for the oversight of a substantial 71% of policies implemented during this timeframe.
During the NAP II (2004−2021), there was a noticeable rise in the volume of policy-making activity by the State Council, evidenced by an increase from 13.7% of proposals during the NAP I to 28.4% in the NAP II. Concurrently, the proportion of policy proposals from the MOH experienced a marked decline, falling from 61.8% to 38.7% from NAP I to NAP II. However, there was a marginal uptick in policies spearheaded by the MOH, rising slightly from 9.2% to 9.6%.
-
Transitioning from the DAP to the NAP, there has been a discernible shift in policy emphasis from targeted interventions and pathways of transmission, along with surveillance and monitoring (decreasing from 24.1% to 12.6%, and from 15.5% to 4.1%, respectively), to an enhanced focus on public education (increasing from 12.1% to 18.9%) and treatment strategies (rising from 1.7% to 6.5%). There was a notable decline in the proportion of policies dedicated to the initiation and reform of government program management mechanisms and staff training, from 12.1% to 3.4%. Significantly, increased attention has been given to scientific researches (increasing from 3.4% to 8.0%) and the coordination between government departments (rising from 1.7% to 5.8%). Additionally, previous deficiencies in areas such as academic conferences and support for individuals impacted by HIV/AIDS have been incrementally addressed over time (increasing from 0.0% to 2.2% and from 1.9% respectively).
During distinct periods, policy emphasis and decision-making priorities shifted markedly. Within the duration of DAP, policies emphasis was placed on targeted interventions to impede transmission routes and other strategies. Conversely, throughout the NAP I, while maintaining a focus on targeted transmission interventions (19.8%) and public education (13.7%), there was an observable uptick in attention to the coordination of governmental departments (9.9%) and bolstering international collaborations (9.9%). Notably, the prevalence of treatment-related policies expanded during this phase, escalating from 1.7% to 6.9%. The subsequent phase, the NAP II, was characterized by a heightened prioritization of public education, representing 21.3% of the policy output. This shift suggests that the SCAWC has begun to effectively fulfill a coordinating role in the formulation of policies.
-
This study conducted a systematic and comprehensive analysis of China’s HIV/AIDS policies over the past four decades, examining the policy shifts and the underlying rationale for these transitions. The investigation delineated two distinct eras in the coordination of China’s HIV/AIDS policies: the DAP and the NAP. This temporal division contrasts with the triphasic categorization — consisting of the entry/introduction phase from 1985 to 1988, the spreading phase from 1989 to 1994, and the expansion phase from 1995 to the present — proposed by previous studies, which were predicated on the number of HIV/AIDS infections (16–19). Consistent with prior studies, our findings indicate a significant transformation in HIV/AIDS policy formulation commencing in 1995 (18,20).
Our investigation revealed that 2004 marked the apex of policy issuance related to HIV/AIDS over the past four decades, with a sustained increase in policy introductions observed from 2005 to 2007. This surge can be attributed to several factors: the 2003 severe acute respiratory syndrome (SARS) outbreak, a significant shift in the political landscape due to the establishment of a new government, and heightened awareness regarding the HIV/AIDS epidemic (6,18,21–22). Advocacy efforts further contributed to a paradigm shift, transforming the discourse from a disease-centric to a human-centric narrative concerning HIV/AIDS (23). While HIV/AIDS assistance and support policies have been in existence since 2003, there remains substantial scope for policy enhancement. There is a pressing need for more nuanced support measures, social services, and programs that align with the actual needs of those impacted by HIV/AIDS.
Transitioning from the DAP to the NAP, there was a notable shift in the perceptions of HIV/AIDS. A more effective policy coordination framework emerged. This evolution progressed from an informal coordination structure exemplified by the Joint Conference in the DAP period, to an institutionalized form of coordination seen with the establishment of the SCAWC during the NAP era. This structured coordination mechanism allowed for government agencies to fulfill their designated roles more effectively.
The initiation of the NAP was precipitated by a marked increase in the incidence of HIV/AIDS in 1995. At that time, reports of the disease had emerged from every province, autonomous region, and municipality under direct central governance (18,22). The swift and extensive propagation of the HIV/AIDS epidemic prompted the government to acknowledge that tackling HIV/AIDS transcended healthcare and necessitated interventions at the societal and political levels. Consequently, the government established a coordination conference to streamline efforts. This aligns with our research findings, which identify 1995 as another pivotal year in the development of HIV/AIDS policy. Notably, the first policy document on HIV/AIDS prevention and control from the State Council, the NSPCA drafted by the Ministry of Health, was ratified and promulgated. The NSPCA laid the foundational policy infrastructure, addressing and reconciling previously conflicting stances among various departments — such as divergent perspectives on condom usage between health and public security agencies — in the nascent stages of AIDS prevention. This policy acted as a catalyst, fostering interdepartmental coordination and paving the way for enhanced HIV/AIDS prevention and treatment strategies.
Since 1982, there has been a significant transition from a casual and sporadic coordination — characterized by mere annual AIDS/STDs prevention and control coordination meetings — to the establishment of a formalized coordination entity. This evolution reflects an increased recognition of the critical role coordination plays. There have been notable structural changes as well; the coordination model evolved from the Coordination Conference System for the Prevention and Control of AIDS and STDs founded in 1996 to the creation of the SCAWC in 2004. Furthermore, AIDS working committees have been instituted at the local government level. Each tier of government now boasts comprehensive mechanisms for the prevention, treatment, and care of HIV/AIDS and has effectively rallied robust support across society and various sectors for the HIV/AIDS response (24).
-
This paper chronicles the evolution of HIV/AIDS policy development and coordination across four decades, with particular emphasis on the transformative years of 1995 and 2004. These years marked significant shifts in the organizational framework, as evidenced by the transition between the DAP and the NAP, and the subsequent progression from the NAP I to the NAP II, concurrent with an unprecedented surge in policy enactments. The restructuring during these periods laid a robust groundwork for a cooperative approach to HIV/AIDS prevention and control, enabling the MOH and various sectors to effectively collaborate. A notable elevation in HIV/AIDS awareness and comprehension emerged between 2003 and 2004, catalyzing a pivotal redirection of policy focus towards the support of individuals impacted by HIV/AIDS. Nevertheless, despite these advancements, current HIV/AIDS care and support mechanisms continue to exhibit significant deficiencies. To address these shortcomings, the development of more inclusive policies is imperative. These policies should be co-designed with the HIV/AIDS community, targeting the enhancement of employment prospects, eradication of stigma, and provision of mental health services. Furthermore, additional research is warranted to ascertain the optimal strategies for the formulation and execution of HIV/AIDS-related policies.
-
No conflicts of interest
-
The authors extend their gratitude to the Hebei Office for Philosophy and Social Sciences, China, for their generous support. We also offer our sincere thanks to the distinguished experts and scholars who enriched this study with their participation in discussions and interviews.
HTML
Data Source
Study Design
Data Analysis
HIV/AIDS Policy Evolution Trends
Policy Focus Areas by Issuing Agencies
Level of Government Agenda by Period
Government Agencies Involved by Period
Evolution of Policy Focus Areas by Period
FootNote
| ① |
|
| Citation: |

|