

 Download:
Download:




-
Breast cancer in females represents one of the most rapidly increasing malignancies in China (1-3). Projections estimate that over 400,000 new diagnoses and over 100,000 fatalities will transpire by 2030 within the nation (4). Consequently, it is crucial to establish targeted intervention strategies for this cancer to avert it from developing into a significant public health issue.
Despite recent advances, there remains a gap in understanding the trends in incidence and mortality rates of female breast cancer in China. The present study aimed to examine these trends from 2003 to 2017, focusing on age groups and geographic distribution. Joinpoint regression modeling and age-period-cohort analyses were employed in this investigation. Additionally, this research can be used to evaluate the effectiveness of current cancer screening initiatives and inform future policy-making in China.
-
The present study analyzed datasets of female breast cancer (C50, ICD-10) from 22 population-based cancer registries in China (11 urban and 11 rural) between 2003 and 2017. The pooled data included 183,521 female breast cancer cases and 41,831 cancer-related deaths from a population of 329,750,392 person-years. Of these, 167,998 cases and 37,341 deaths were from urban areas with 274,073,539 person-years, and 15,523 cases and 4,490 deaths were from rural areas with 55,676,853 person-years.
Given the rarity of female breast cancer among individuals below 20 years of age, data from this population were excluded from subsequent analyses. Incidence and mortality rates were computed using 5-year age intervals (20–24, 25–29, ..., 80–84, ≥85) and stratified by 5-year periods (2003–2007, 2008–2012, 2013–2017) and geographical classification (urban and rural).
-
The age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) were calculated utilizing Segi’s world standard population. Joinpoint regression analysis was conducted for trend examination, and the annual percent changes (APC) and average annual percent change (AAPC) were reported. The age-period-cohort effects were analyzed using the intrinsic estimator method, and risk ratios were provided. Statistical analyses were carried out with Stata (version 13.0, Stata Corporation, College Station, Texas, USA) and Joinpoint software (version 4.6.0.0, Applications Branch, National Cancer Institute, Bethesda, USA).
-
In all regions, the ASIR for female breast cancer in individuals over 20 years old increased from 46.34 per 100,000 in 2003 to 68.78 per 100,000 in 2017, with an AAPC of 2.5% [95% confidence interval (CI): 2.0%–2.9%]. The ASIR was higher in urban areas compared to rural areas.
The ASIR for female breast cancer demonstrated a significant increase across most age groups between 2003 and 2017. However, an exception was observed in the urban 50–64 age group, where the ASIR increased rapidly from 2003 to 2008 (APC=4.5%, 95% CI: 3.4%–5.7%, P<0.001). Following this period, the upward trend slowed between 2008 and 2017 (APC=1.5%, 95% CI: 1.0%–1.9%, P<0.001). Notably, in comparison to urban areas, the ASIR experienced a faster increase in rural areas across all age groups. The most prominent rise was observed in the 20–34 age group in rural areas, with an APC of 9.0% (95% CI: 7.0%–11.0%, P<0.001) throughout the entire period (Figure 1A, 1B, 1C). Corresponding trend analysis results for incidence rates can be found in
Supplementary Table S1 . Figure 1.
Figure 1.Trends in incidence and mortality rates of female breast cancer by age group and area, 2003–2017. (A) Incidence rates across all areas. (B) Incidence rates in urban settings. (C) Incidence rates in rural settings. (D) Mortality rates across all areas. (E) Mortality rates in urban settings. (F) Mortality rates in rural settings.
-
Across all regions, the ASMR for females with breast cancer aged 20 and above experienced an increase from 11.12 per 100,000 in 2003 to 11.67 per 100,000 in 2017, exhibiting an AAPC of 0.9% (95% CI: 0.4%–1.3%).
For females over 20 years old, the ASMR increased more rapidly in rural areas (APC=2.4%, 95% CI: 1.7%–3.2%, P<0.001) compared to urban areas (APC=0.6%, 95% CI: 0.2%–1.1%, P=0.013). When examining the data by age group, the ASMR for the 20–34 age group exhibited stability in both urban and rural areas from 2003 to 2017. The ASMR for the 35–49 age group in urban areas declined between 2003 and 2009 (APC=−3.6%, 95% CI: −6.4% to −0.7%, P=0.020) and then stabilized. In contrast, the ASMR for the 50–64 age group in rural areas and the over-65 age group in both areas showed significant increases, with the most substantial increase observed in the over-65 age group in rural areas (APC=4.9%, 95% CI: 2.8%–7.0%, P<0.001) (Figure 1D, 1E, 1F). The corresponding mortality rate trend analyses are provided in
Supplementary Table S2 . -
In urban areas, the age distribution trends of female breast cancer incidence rates were consistent across three study periods. The ASIR exhibited a rapid increase starting from the 20–24 age group. During 2003–2012, a plateau in the incidence rate was observed between the 45–49 and 70–74 age groups, followed by a rapid decline. In the period of 2013–2017, the incidence rate continued to increase, albeit at a slower pace, beginning at the 45–49 age group and peaking within the 60–64 age group. The rate then exhibited a gradual decrease until the 70–74 age group and subsequently declined rapidly (Figure 2B).
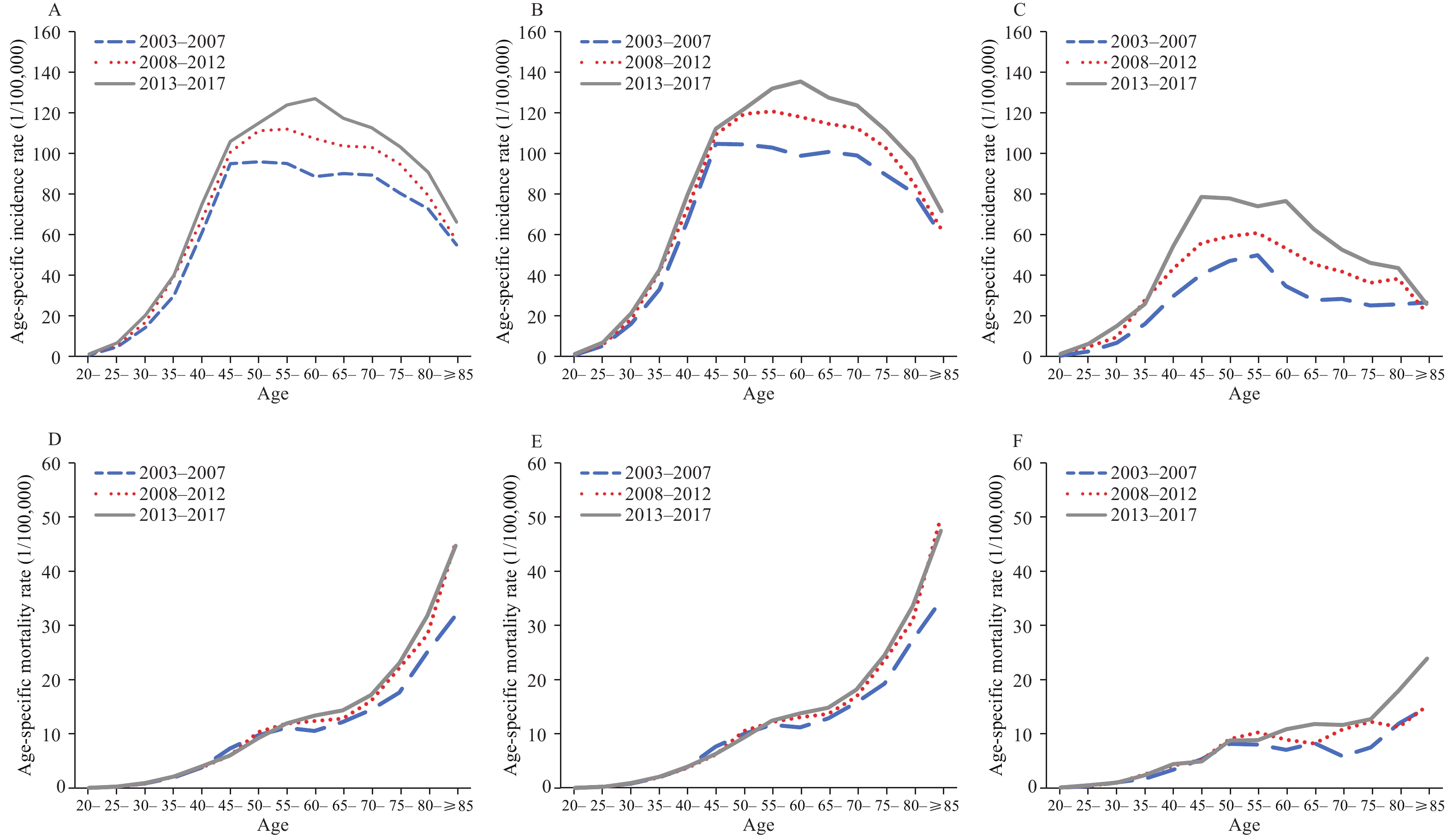 Figure 2.
Figure 2.The age-specific incidence and mortality rates of female breast cancer, by time period and area. (A) Incidence rates in all areas. (B) Incidence rates in urban areas. (C) Incidence rates in rural areas. (D) Mortality rates in all areas. (E) Mortality rates in urban areas. (F) Mortality rates in rural areas.
Note: Each line represents the connection of age-specific rates for a 5-year period.In rural regions, the ASIR reached its peak within the 55–59 age group during the periods of 2003–2007 and 2008–2012. However, between 2013 and 2017, the rate experienced a plateau spanning from the 45–49 age group to the 60–64 age group (Figure 2C).
The incidence rates showed an increase for cohorts from 1933 to 1988 (ages 25–74) in urban areas, and for cohorts from 1923 to 1993 (ages 20–84) in rural areas (Figure 3A, 3B).
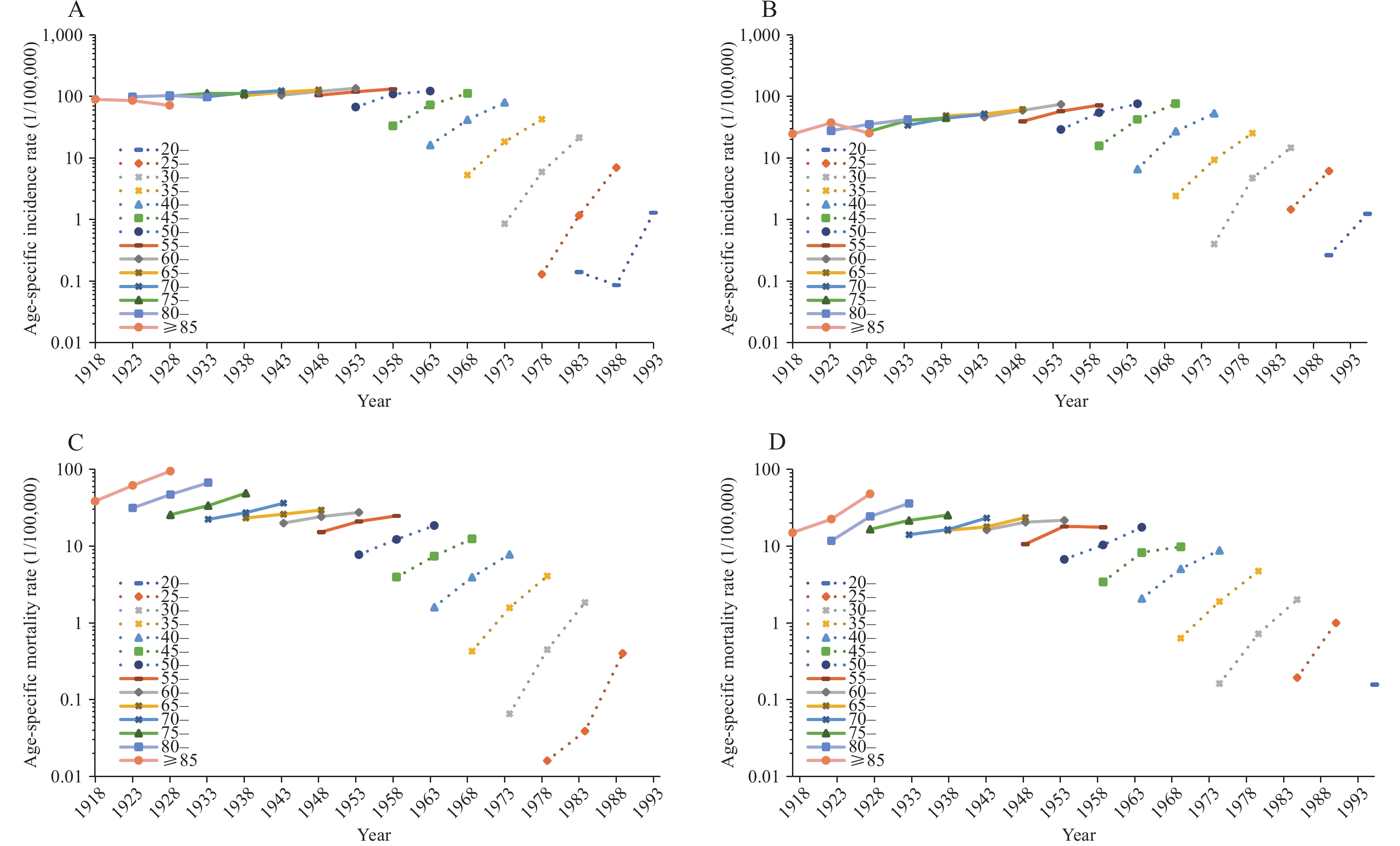 Figure 3.
Figure 3.The birth cohort-specific incidence and mortality rates of female breast cancer, by area. (A) Incidence rates in urban areas. (B) Incidence rates in rural areas. (C) Mortality rates in urban areas. (D) Mortality rates in rural areas. Results were not shown in age group 20–24 if the age-specific rate is 0.
Note: Each line represents the connection of cohort-specific rates for a 5-year age group. -
In both urban and rural settings, there is a positive association between age and ASMRs, with rates increasing as age increases (Figure 2E, 2F).
The mortality rates exhibits an increase across all cohorts in both urban and rural settings (Figure 3C, 3D).
-
The age, period, and cohort effects exhibited similarity across urban and rural areas. In both regions, the age effect on female breast cancer incidence rates increased significantly from the 20–24 age group, reaching a peak in the 45–49 age group. Subsequently, the age effect decreased gradually within the following age groups. As for mortality rates, the age effect escalated significantly within the 20–24 age group, peaking in the 50–54 age group. A slight decrease occurred thereafter, followed by a resurgence in the 65–69 age group in urban areas and the 70–74 age group in rural areas (Figure 4).
 Figure 4.
Figure 4.The result of age-period-cohort analysis of incidence and mortality rates of female breast cancer, by area. (A) Incidence rates in urban areas. (B) Incidence rates in rural areas. (C) Mortality rates in urban areas. (D) Mortality rates in rural areas. ote:Blue solid and dash lines represent the age effect and 95% confidence interval. Orange solid and dash lines represent the period effect and 95% confidence interval. Pink solid and dash lines represent the cohort effect and 95% confidence interval.
The incidence and mortality rates demonstrated a period effect, with increases observed from 2003 to 2017.
In urban regions, there was a consistent decline in the cohort effect on both incidence and mortality rates. Conversely, in rural areas, the cohort effect on incidence rates exhibited a rapid decrease, followed by a minor resurgence observed among those born between 1983 and 1992. As for mortality rates in rural areas, the cohort effect initially declined, but experienced a slight increase for the cohort born between 1928 and 1937, and subsequently showed a continuous decrease thereafter (Figure 4).
-
Age effect: The present study revealed that the incidence rate of female breast cancer was the highest among the age group of 45–70 years, consistent with global observations (5). In this investigation, the peak age effect for female breast cancer incidence occurred in the 45–49-year-old group. Luan et al. (6) assessed the age-period-cohort effects on female breast cancer incidence in Hong Kong, Shanghai, and White and Black populations in Los Angeles. Although the age effect also peaked in the 45–49-year-old group in Shanghai, distinct patterns were observed in the other three populations. These diverse age effect patterns across various populations might be attributable to the potential differences in the prevalence of tumor-related genes (7).
Ding et al. (8) discovered a rapid increase in breast cancer mortality rates from the 20–24 age group to the 45–49 age group, followed by a slower rate of increase. Wang et al. (9) noted that the age effects of breast cancer mortality plateaued in the 55–59 age group and then gradually declined in Japan and Korea, while the age effect consistently increased with age in Singapore. In the present study, a small peak in the female breast cancer mortality rates was observed within the 50–54 age group. Further investigation is necessary to determine the reasons for the elevated risk in this particular age group.
Period effect: Our study identified increasing period effects in female breast cancer incidence and mortality rates from 2003 to 2017, aligning with findings from previous research (8-10). This observation suggests that socioeconomic transformations and modernized lifestyle changes may constitute the primary factors contributing to the rise in breast cancer incidence and mortality in China.
Screening strategies are crucial influencing factors for incidence and mortality trends in breast cancer. Krishnamoorthy et al. (11) conducted an analysis of worldwide breast cancer incidence rate trends across various regions. Their findings indicated that the Americas had the highest breast cancer incidence, but it was the one region in which the incidence rate had been declining. Likewise, the period effect in the Americas displayed a decreasing trend. These findings suggest that the breast cancer screening programs in the Americas have reached a saturation point, and their health benefits have become evident. However, due to the limited coverage of screening programs in China, the period effect has not yet been reversed. Drawing on the experiences of the Americas, it can be predicted that the period effect and the ASIR for breast cancer will continue to rise for an extended period in China.
Cohort effect: Our research identified a decreasing cohort effect in incidence and mortality rates for female breast cancer, consistent with findings from previous studies (6,8–10). This decline in cohort effect suggests that older birth cohorts face a higher risk of developing female breast cancer than younger cohorts. The possible reasons for this reduction may include healthier living habits and enhanced health awareness among younger generations, along with improvements in public health policies and clinical diagnosis and treatment options in recent years.
It is important to note, however, a slight upsurge in cohort effect was observed among younger populations in rural areas of China. This reversal may result from an increased exposure to emerging risk factors, such as sedentary lifestyles (12), changes in reproductive behaviors (e.g., delayed first childbirth, nulliparity, and oral contraceptive pill use), and diminished breastfeeding practices (13). These factors come in addition to well-established risks such as physical inactivity, excessive body weight, and diabetes (14).
The early diagnosis rate for female breast cancer in China was significantly higher than that observed for other types of cancer (15). Our data further revealed that between 2003 and 2017, the mortality rate for female breast cancer increased at a slower pace than the incidence rate. This evidence suggests that current screening programs have yielded substantial benefits through early detection and treatment. However, it is critical to recognize that effective primary prevention strategies for addressing new risk factors remain limited. Without them, reducing breast cancer incidence in the short term may be unattainable. As such, there is a pressing need to develop comprehensive public health intervention strategies, particularly for younger generations and vulnerable populations.
In the current study, we utilized continuous surveillance data from 22 cancer registries spanning 2003 to 2017, offering a more accurate depiction of trends in rates as compared to alternative multi-sectional datasets. Additionally, the use of ICD-10 coding for cancer registry data enhances the precision of our analysis. Nonetheless, some limitations exist within this dataset, primarily due to its restricted population coverage, particularly in rural areas. This results in increased fluctuation within trends and broader 95% CI for risk ratio point estimation. Furthermore, the observation period in this study is relatively shorter than those found in research conducted in other countries.
In conclusion, the present study examined the period from 2003 to 2017 and found increasing incidence rates of breast cancer across all age groups and geographic locations. However, rising mortality rates were observed predominantly among women over 50 years old, particularly in rural areas. These trends can be primarily attributed to period effects, while cohort effects generally decreased. Notably, a slight upward trend was detected for younger generations in rural regions. Consequently, it is crucial to adjust and refocus current intervention strategies for female breast cancer in China to adequately address the growing burden of this disease.
-
No conflicts of interest.
-
Staffs of 22 population-based cancer registries including Beijing; Cixian County, Hebei Province; Dalian and Anshan cities, Liaoning Province; Nangang District, Heilongjiang Province; Shanghai; Qidong City, Huai’an District, and Yangzhong City, Jiangsu Province; Hangzhou City, Jiaxing City, Jiashan County, and Haining City, Zhejiang Province; Changle District, Fujian Province; Linqu County and Feicheng City, Shandong Province; Linzhou City, Henan Province; Wuhan City, Hubei Province; Guangzhou, Sihui, and Zhongshan cities, Guangdong Province; and Yanting County, Sichuan Province.
HTML
Cancer Registry Data
Statistical Analysis
Trends in Incidence Rate
Trends in Mortality Rate
Trends in Age Distribution of Female Breast Cancer Incidence
Trends in Age Distribution of Female Breast Cancer Mortality
Results of Age-Period-Cohort Models
| Citation: |

|