

 Download:
Download:




-
Cervical cancer, the fourth most common cancer and the fourth leading cause of cancer death in women worldwide (1), is preventable through effective screening and vaccination. Human papillomavirus (HPV) testing is now recommended as the primary method in cervical cancer screening (2). HPV-16 and 18 are the most carcinogenic high-risk (hrHPV) subtypes and account for approximately 70% of cervical cancers (3). Understanding the prevalence patterns of different hrHPV subtypes is important to identify target populations for screening and vaccination. However, the age-specific prevalence of different hrHPV subtypes remains unclear among women in rural areas in southern China. A total of 159,251 women aged 35–64 years who participated in a cervical cancer screening program in rural areas in Guangzhou City, Guangdong Province, China, from 2019–2021 were included in this population-based study. All women received the hrHPV test using Roche Cobas 4800 (Roche Molecular Systems, Pleasanton, USA). We found that the prevalences of HPV-16, 18, and the other 12 hrHPV types were 0.71%, 0.34%, and 4.50%, respectively, among rural women in Guangzhou. We observed the prevalence of HPV-16 declined in the age group of 35–49 years and increased by age group afterwards, whereas the prevalence of the other 12 hrHPV subtypes increased with age from 40–44 years old (Ptrend<0.01), but there was no evident trend for HPV-18 prevalence across the age groups (Ptrend=0.70). Our findings might have implications in the identification and follow-up for high-risk population of hrHPV infection.
This study was based on a population-based cervical cancer screening program covering all seven rural administrative districts in Guangzhou during 2019–2021. All screened women aged 35–64 years with rural registered permanent residence in Guangzhou were included in the study. All women received a gynecological examination and the hrHPV test using Roche Cobas 4800 (Roche Molecular Systems, Pleasanton, USA) HPV Detection (Cobas). Cobas could specifically identify HPV-16 and HPV-18 while concurrently detecting the other 12 hrHPV types (HPV-31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68). All women provided written informed consent before screening. Age-specific prevalence of hrHPV infection was calculated by five-year age groups. The Cochran-Armitage test was used to examine the overall linear trends of the prevalence of hrHPV subtypes across age groups. The two-sided Poisson test was used to compare the prevalence ratios (PR) across age-groups and calculate the 95% confidence interval (CI). Stratified analyses of prevalence of hrHPV subtypes were performed among women who were first time to participate in HPV screening or not. Analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA) or R (version 4.0.3; R Core Team, Vienna, Austria).
A total of 159,251 women aged 35–64 years (mean: 46.51 years) were included in the study. Women aged 35–39 years old accounted for 23.18% of the participants while 5.04% of women were 60–64 years old. Of the included participants, 8,465 (5.32%) women were detected as hrHPV positive, with 1,130 (0.71%) positive for HPV-16, 538 (0.34%) positive for HPV-18 and 7,168 (4.50%) positive for the other 12 hrHPV types (Table 1). Among women who tested as hrHPV positive, 13.35% were positive for HPV-16, 6.36% for HPV-18, and 84.68% for the other 12 hrHPV subtypes.
Infection patterns No. of positive Prevalence (%) (95% CI) Proportion of hrHPV (%) Any types of infection Any hrHPV subtypes 8,465 5.32 (5.21–5.43) 100.00 Any HPV-16 1,130 0.71 (0.67–0.75) 13.35 Any HPV-18 538 0.34 (0.31–0.37) 6.36 Any pooled 12 hrHPV types 7,168 4.50 (4.40–4.60) 84.68 HPV-16 or HPV-18 1,651 1.04 (0.99–1.09) 19.50 Co-infection HPV-16 + Other hrHPV types* 249 0.16 (0.14–0.18) 2.94 HPV-18 + Other hrHPV types† 134 0.08 (0.07–0.10) 1.58 HPV-16 + 18 12 0.008 (0.004–0.014) 0.14 HPV-16 +18 + Pooled 12 hrHPV types 5 0.003 (0.001–0.007) 0.06 Abbreviation: hrHPV=high-risk human papillomavirus, CI=confidence interval.
* Other hrHPV types means pooled 12 hrHPV types or HPV-18.
† Other hrHPV types means pooled 12 hrHPV types or HPV-16.Table 1. The prevalence of hrHPV subtypes in rural Guangzhou, China, 2019–2021.
Age-specific prevalence for hrHPV subtypes is shown in Table 2. The prevalence of HPV-16 slightly declined from 35–49 years group and increased with age afterwards, indicating an overall upward trend (Z=−3.19, Ptrend<0.01, Figure 1). Highest prevalence of HPV-16 was observed among women of 60–64 years, with a PR of 1.34 (95% CI: 1.02–1.73) compared with those of 35–39 years (Table 2). Women at 60–64 years also had the highest prevalence of HPV-18, but there was no evident trend for HPV-18 prevalence across the age groups (Z=−0.39, Ptrend=0.70). The other 12 hrHPV subtypes also had an increasing prevalence along with age (Z=−6.16, Ptrend<0.01), with the highest prevalence observed among women at 60–64 years (PR, 1.39; 95% CI: 1.26–1.54). Stratified analysis showed similar age-specific prevalence patterns between women undergoing HPV screening for the first time and those who had participated before (
Supplementary Figure S1 ).Age group Total participants
(%)HPV-16 HPV-18 Pooled 12 hrHPV No. of positive Positive rate (%)
(95% CI)Prevalence ratio (95% CI) No. of positive Positive rate (%)
(95% CI)Prevalence ratio (95% CI) No. of positive Positive rate (%)
(95% CI)Prevalence ratio (95% CI) 35–39 36,914 (23.18) 262 0.71 (0.63–0.80) 1.00 136 0.37 (0.31–0.44) 1.00 1,623 4.40 (4.19–4.61) 1.00 40–44 29,917 (18.78) 190 0.64 (0.55–0.73) 0.89 (0.74–1.08) 93 0.31 (0.25–0.38) 0.84 (0.64–1.11) 1,243 4.15 (3.93–4.39) 0.94 (0.88–1.02) 45–49 34,974 (21.96) 206 0.59 (0.51–0.68) 0.83 (0.69–1.00) 104 0.30 (0.24–0.36) 0.81 (0.62–1.05) 1,511 4.32 (4.11–4.54) 0.98 (0.92–1.05) 50–54 31,151 (19.56) 232 0.75 (0.65–0.85) 1.05 (0.88–1.26) 112 0.36 (0.30–0.43) 0.98 (0.75–1.26) 1,364 4.38 (4.16–4.61) 1.00 (0.93–1.07) 55–59 18,275 (11.48) 164 0.90 (0.77–1.05) 1.26 (1.03–1.54) 53 0.29 (0.22–0.38) 0.79 (0.56–1.09) 936 5.12 (4.81–5.45) 1.16 (1.07–1.26) 60–64 8,020 (5.04) 76 0.95 (0.75–1.19) 1.34 (1.02–1.73) 40 0.50 (0.36–0.69) 1.35 (0.93–1.94) 491 6.12 (5.61–6.67) 1.39 (1.26–1.54) Total 159,251 1,130 0.71 (0.67–0.75) – 538 0.34 (0.31–0.37) – 7,168 4.50 (4.40–4.60) – Abbreviation: hrHPV=high-risk human papillomavirus; CI=confidence interval.
“–” means not applicable.Table 2. The prevalence of HPV-16, HPV-18, and the other 12 hrHPV subtypes by age group during 2019–2021 in rural Guangzhou, China (N=159,251).
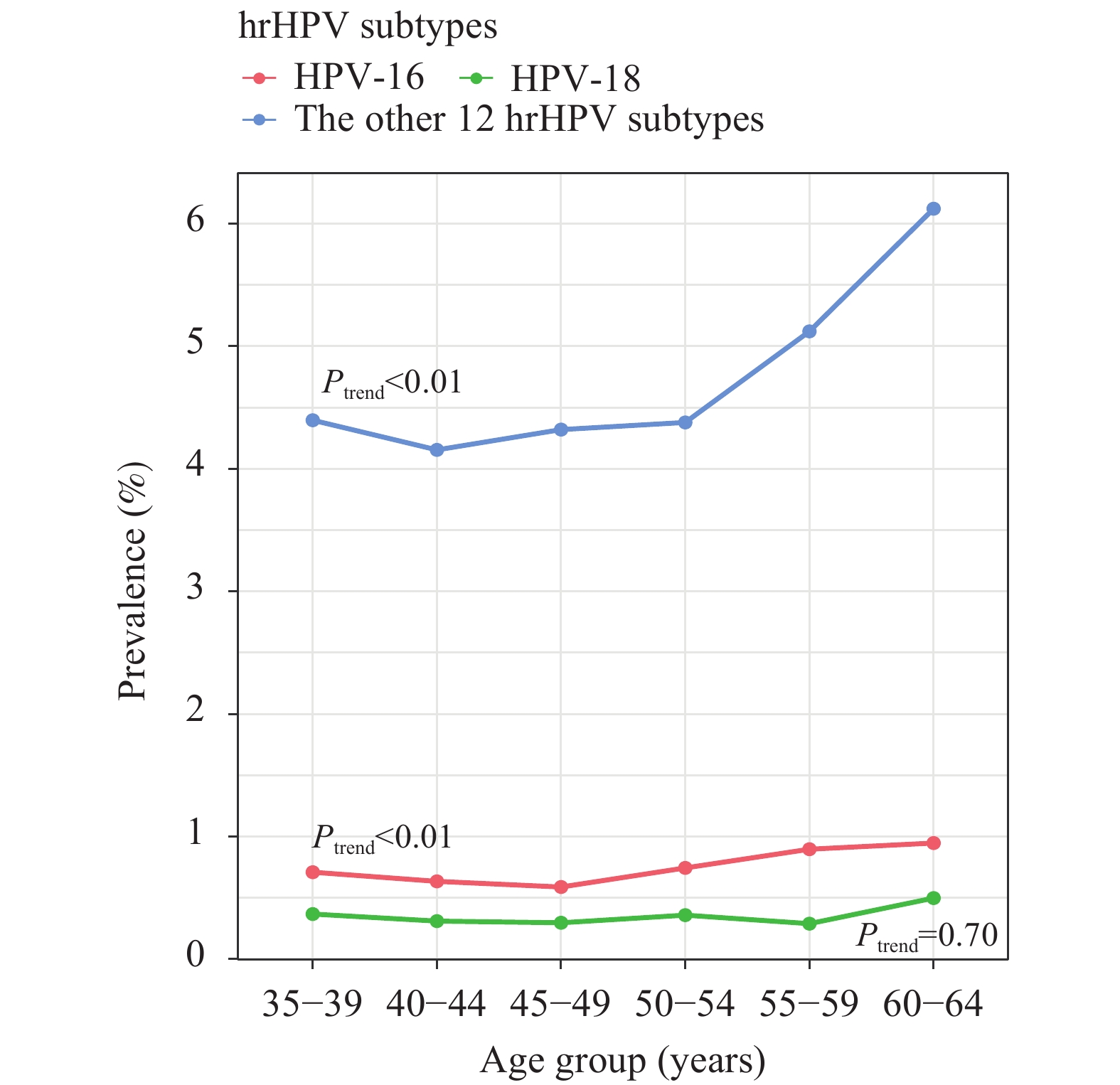 Figure 1.
Figure 1.The prevalence and trend of hrHPV subtypes by age group during 2019–2021 in rural Guangzhou, China (N=159,251).
Abbreviation: hrHPV=high-risk human papillomavirus. -
In this study, we characterized the prevalence pattern of hrHPV subtypes among rural women in Guangzhou, China. We found the prevalences of HPV-16, HPV-18, and the other 12 hrHPV subtypes were 0.71%, 0.34%, and 4.50%, respectively. An overall upward trend in prevalence was observed for both HPV-16 and the other 12 hrHPV across age groups. Although there was no significant age trend for HPV-18, women at 60–64 years appeared to have the highest prevalence of HPV-18.
It has been well documented that HPV-16 and HPV-18 have a higher likelihood of persistence and progression to cervical lesions compared with other oncogenic types, accounting for approximately 70% of cervical cancers globally (3). Understanding the prevalence of hrHPV subtypes is beneficial for decision making for both screening strategies and vaccination. The distribution of HPV-16 and HPV-18 in general population varies across continents: 5.8% and 2.3% in northern America, 4.8% and 0.9% in Europe, and 2.5% and 1.4% in Asia (mostly from India) (4). Even within China, the prevalence of hrHPV subtypes varies among different regions. For example, the prevalence of HPV-16 ranges from 0.71% in Guangdong Province to 3.62% in Zhejiang Province, whereas the prevalence of HPV-18 ranges from 0.28% in Jiangxi Province to 1.48% in Zhejiang Province (5-7). These differences in hrHPV prevalence across regions could be due to different HPV testing approaches or different age structure of the population under investigation and might reflect actual geographic variations in hrHPV prevalence. Using the same method (i.e., Cobas) for a close age-distributed population (older than 30 years old) as this study, Guo revealed rates of 0.71% and 0.30% for HPV-16 and HPV-18 among a small sample (n=986) in Guangdong Province (6), while another study in Hubei Province (n=313,704) found that the prevalences of HPV-16 and HPV-18 were 1.51% and 0.46%, respectively (8).
This study found that different hrHPV subtypes presented different patterns for age distribution. It has been reported that the prevalence of HPV-16/18 gradually increased among 35–50 age group in general population in Guangdong Province, China (7). However, the prevalence of HPV-16 decreased to the lowest point in the 45–49 age group and then went upward in the current study. As for the prevalence of the other 12 hrHPV subtypes, a significant increase across age groups was observed in the rural women of Guangzhou. Another study also found a similar trend for HPV-52 and HPV-58 in Guangdong Province, China, which are the most common types in the other 12 hrHPV subtypes (7).
The findings of this study might have important implications in public health. First, the variability in prevalence patterns for different hrHPV subtypes across age groups indicates that women at different ages might have different risk factors for hrHPV infection. It provides a better understanding for the epidemiological characteristics of hrHPV in rural Guangzhou. Second, we found that women at an older age have a higher prevalence of HPV-16 and the other 12 hrHPV subtypes than those at a younger age. This suggests that elderly women deserve additional concern because most national guidelines recommend stopping cervical cancer screening at age 65 (9). Whether the high prevalence of hrHPV subtypes also translates into a higher cervical intraepithelial neoplasia burden in elderly women needs further investigation.
Although this study had the advantage of a large sample size, limitations remain. First, we are unable to identify the prevalence of each of the other 12 hrHPV because Cobas detects them concurrently. Second, pathological data were not available; thus, the association between HPV subtypes and cervical cancer or precancerous lesions could not be examined. Furthermore, only data from Guangzhou were included in this study, it cannot be extrapolated to the whole rural area of China. Multiarea data are needed to characterize the prevalence of hrHPV subtypes in rural China.
In conclusion, we found that different hrHPV subtypes had different age-specific prevalence patterns and women at an older age had significantly higher prevalence of HPV-16 and the other 12 hrHPV subtypes. This information is helpful for better understanding the epidemiological characteristics of hrHPV subtypes in rural Guangzhou and provides a scientific basis for identification and follow-up of high-risk populations. Further investigations are warranted to investigate the prevalence and health effects of HPV-16 and the other 12 hrHPV subtypes in elderly women.
-
We thank Professor Gendie Lash for editing English language on our paper.
HTML
| Citation: |

|