

 Download:
Download:




-
Hong Kong Special Administrative Region (SAR), China and Singapore have been facing the Omicron epidemic since January 2022. Despite their similar socioeconomic statuses, Hong Kong SAR, China encountered a higher case fatality ratio (CFR) accompanied by an overwhelmed medical system compared to Singapore. This study collected and compared the CFRs, vaccination coverage, infection rate, and medical resources occupancy rates from the two places. The vaccine coverage rates and CFRs in 52 Omicron variant dominated countries and regions were also collected and multiple linear regressions were used to explore associations. The random forest (RF) method was additionally used to estimate the importance of factors contributing to CFRs. The CFR in Hong Kong SAR, China was larger than in Singapore (0.53% vs. 0.06%), especially for people ≥70 years (4.46% vs. 0.48%). Correspondingly, the vaccine coverage was lower in Hong Kong SAR, China than in Singapore (full vaccine coverage for total population: 76.15% vs. 92.00%; for people ≥70 years: 56.82% vs. 95.00%). Based on the data from Omicron variant dominated countries and regions, a negative association between vaccine coverage and CFR was observed. The RF model indicated that full vaccination and ≥1 dose vaccination coverages were the top two contributing factors to CFR. These findings call on people without complete coronavirus disease 2019 (COVID-19) vaccinations, especially the elderly, to get any type of accessible vaccine, which could save lives.
Since the emergence of Omicron variant, due to its heightened transmissibility, the whole world has been suffering a new wave of the COVID-19 pandemic (1). As finance and trade centers with high international connectivity, Hong Kong SAR, China and Singapore have been experiencing a considerable increase in COVID-19 cases since January 2022. According to the Government of Hong Kong SAR, China, the epidemic was overwhelming the medical system with a relatively high CFR (2), while Singapore seemed to manage its epidemic within the capacity of its medical system contributing to a lower CFR (3). As we know, Hong Kong SAR, China and Singapore share many similar characteristics, such as developed economy, freeport international trade, and a similar population density. However, it is unclear why there is such a stark difference in CFR between the two locations. This study aims to explore this important issue, which could provide significant implications for China to develop and adjust future COVID-19 prevention strategies.
Hong Kong SAR, China had been applying the zero-COVID policy using strict non-pharmaceutical interventions (NPIs) such as border quarantine, social distancing, and mask wearing, and achieved low cases during the first four waves of epidemic. Unfortunately, several infected flight staff did not obey the quarantine rule and entered the community, which was the suspected origin of the Omicron variant epidemic in Hong Kong SAR, China. Because of the superior transmissibility of Omicron variant, the delayed identification, and the control of all infected people, the epidemic rapidly expanded. Together with low vaccination coverage among the elderly, the imperfect tiered diagnosis, and treatment strategy at the early stage, more severe cases may occur and a few patients with mild symptoms may occupy the hospital beds, which lead to overwhelmed medical systems.
Since the emergence of the first case of COVID-19 in January 2020 in Singapore, its containment strategy had been applied until August 2021, when 78% of its population had been vaccinated with at least one dose. Since then, Singapore has continued to promote COVID-19 vaccination and tried to transition to “co-existence with virus” strategy by gradually lifting NPI restrictions. Singapore has also been optimizing the tiered diagnosis and treatment strategy, which effectively relieved the pressures on the medical system.
CFRs, vaccination coverage, infection rate, medical resources occupancy rates for COVID-19, and other comparative variables, including age structure, the number of swab tests, and prevalence of chronic diseases were obtained and calculated from the Government of the Hong Kong SAR, China and Singapore. The detailed source websites were presented in the footnotes of tables and figures.
To investigate the effects of vaccination coverage after controlling for confounding factors, we collected the data of 52 Omicron dominated countries and regions (Omicron proportion ≥90%) from Our World in Data (https://ourworldindata.org/). Nine explanatory variables, including full vaccination, ≥1 dose, booster vaccination, gross domestic product (GDP) per capita, population density, hospital beds per 1,000 people, human development index, proportion of people aged 70 and older, and cardiovascular mortality per 100,000 people were collected. One dependent variable (CFR) was collected. The detailed definitions of these variables are presented in
Supplementary Table S1 . Due to the 28-day efficacy assessment period (4), the proportion of people with at least one dose, with full vaccination, with booster vaccination before February 7, 2022 were collected and then averaged for analysis.Multiple linear regression models were employed to explore the effects of vaccination coverage (full vaccination, ≥1 dose, and booster vaccination) on CFR separately, after controlling for potential confounding variables. In addition, a random forest (RF) regression model was used to qualitatively assess the feature importance of nine explanatory variables contributing to CFR. RF regression analysis, a tree-based machine learning algorithm, works well with multicollinearity and nonlinear problems between predictors and makes decisions by constructing a multitude of decision trees (5,000 trees in this study) for training the data included in a model (5–6). Predictions for each variable are aggregated across all trees and percentage increase in mean square error (%IncMSE) is calculated, which indicates how much the model accuracy decreases if that variable were omitted.
All statistical analyses were performed using R software (version 4.0.5, R Foundation for Statistical Computing, Vienna, Austria). A two-sided P value of <0.05 represented statistically significant.
Table 1 shows that from December 31, 2021 to March 22, 2022, the CFR of COVID-19 in Hong Kong SAR, China (0.58%; age standardization: 0.53%) is much larger than in Singapore (0.05%; age standardization: 0.06%). The CFRs increase with the rise of age in both Hong Kong SAR, China and Singapore, and in most age groups, CFRs were higher in Hong Kong SAR, China than in Singapore, especially for people ≥70 years.
Age group
(years)Hong Kong SAR, China Singapore* Vaccine coverage (%) Number of
casesNumber of
deathsCFR (%) Vaccine coverage (%) Number of
casesNumber of
deathsCFR (%) ≥1 dose Full vaccination† Booster vaccination§ ≥1 dose Full vaccination† Booster vaccination§ 0–19 66.43 34.98 3.97 105,847 11 0.01% 65.00 61.00 – 143,320 0 0.00 20–39 93.77 86.76 31.88 304,771 25 0.01% 98.00 98.00 – 251,281 0 0.00 40–59 98.52 92.67 50.01 353,560 218 0.06% 98.00 98.00 – 199,263 12 0.01 60–69 89.77 81.24 43.97 156,183 521 0.32% 97.00 97.00 – 82,019 38 0.05 ≥70 70.93 56.82 24.61 118,570 5,371 4.46% 96.00 95.00 – 63,154 300 0.48 Total 87.61 76.15 34.50 1,038,931 6,146 0.53¶
(0.36–0.70)**93.00 92.00 71.00 739,037 350 0.06¶
(0.01–0.18)**Note: CFR, vaccination coverage was obtained and calculated from the Government of the Hong Kong SAR, China (https://www.coronavirus.gov.hk/eng/index.html) and Ministry of Health in Singapore (https://www.moh.gov.sg/).
“–” means data not available.
Abbreviation: CFR=case fatality ratio; SAR=Special Administrative Region.
* The proportion of inactivated vaccination is just 3.52% in Singapore (obtained from: https://www.hsa.gov.sg/COVID19-vaccines-safety-updates).
† Full vaccination in Hong Kong SAR, China refers to people with 2 doses inactivated or mRNA vaccine in this study. Full vaccination in Singapore refers to people with 2/3 doses inactivated vaccine or 2 doses mRNA vaccine.
§ Booster vaccination in Hong Kong SAR, China refers to the people with 3 doses inactivated or mRNA vaccine. Booster vaccination in Singapore refers to the people with “2/3 doses inactivated vaccine + 1 dose mRNA vaccine” or “3 doses mRNA vaccine”.
¶ Age standardized CFR (the number of age-specific infections and infected related deaths in Hong Kong SAR, China and Singapore were combined as a reference group).
** 95% confidential interval.Table 1. The comparison of CFR and vaccination coverage in Hong Kong SAR, China and Singapore, by age group — December 31, 2021 to March 22, 2022.
As of March 22, 2022, the full vaccination and booster coverage in Hong Kong SAR, China was 76.15% and 34.50%, respectively, which is much lower than in Singapore with 92.00% full vaccination and 71.00% with a booster vaccination. Especially for people aged ≥70 years in Hong Kong SAR, China, the full vaccination rates are far lower (56.82%) than in Singapore (95.00%).
Table 2 presents the CFRs by vaccination status and age groups. The CFRs of cases with full vaccination were far lower than those with partial vaccination, especially for the elderly. In Singapore, the CFR for people ≥70 years ranges 7.20%–16.00% for non-fully vaccinated cases, 0.76%–2.80% for fully vaccinated cases, and 0.08%–0.41% for booster vaccinated cases. The CFRs of fully vaccinated cases were also lower than those without full vaccination in Hong Kong SAR, China.
Age group
(years)CFR in Hong Kong SAR, China* (%) CFR in Singapore† (%) Non-full
vaccination§Full
vaccination¶Booster
vaccination**Non-full
vaccination§Full
vaccination¶Booster
vaccination**0–9 0.01 0.00 – 0.00 0.00 0.00 10–19 0.01 0.00 – 0.00 0.00 0.00 20–29 0.03 0.00 – 0.02 0.00 0.00 30–39 0.04 0.00 – 0.04 0.00 0.00 40–49 0.12 0.01 – 0.12 0.01 0.00 50–59 0.44 0.03 – 0.89 0.06 0.00 60–69 0.99 0.08 – 2.90 0.20 0.03 70–79 2.81 0.38 – 7.20 0.76 0.08 ≥80 11.25 3.22 – 16.00 2.80 0.41 Total 1.69††,§§ 0.10††,§§ – 2.92
(0.26–8.72)††0.14
(0.01–0.53)††0.03¶¶ Note: CFR with different vaccination statuses were obtained and calculated from the Government of the Hong Kong SAR, China (https://www.coronavirus.gov.hk/eng/index.html) and Ministry of Health in Singapore (https://www.moh.gov.sg/).
“–” means data not available.
Abbreviation: CFR=case fatality ratio; SAR=Special Administrative Region.
* The CFR in Hong Kong SAR, China from December 31, 2021 to March 22, 2022.
† The CFR in Singapore from May 1, 2021 to February 28, 2022.
§ “Non-full vaccination” refers to people without vaccination and with 1 dose vaccination.
¶ Full vaccination in Hong Kong SAR, China refers to people with 2 doses inactivated or mRNA vaccine in this study. Full vaccination in Singapore refers to people with 2/3 doses inactivated vaccine or 2 doses mRNA vaccine.
** Booster vaccination in Hong Kong SAR refers to the people with 3 doses inactivated or mRNA vaccine. Booster vaccination in Singapore refers to the people with “2/3 doses inactivated vaccine + 1 dose mRNA vaccine” or “3 doses mRNA vaccine.
†† Age standardized CFR (the number of age-specific infections and infected related deaths in Hong Kong SAR, China were used as a reference group; the age-vaccinated status-specific number of infections of Singapore could not be obtained).
§§ The confidence intervals were not presented because the population in Hong Kong SAR, China was used as a reference group.
¶¶ The standardized total CFR of booster vaccinated infectors could not be calculated because the age-specific number of booster vaccinated infectors in Hong Kong SAR, China and Singapore could not be obtained.Table 2. The CFR with different vaccination statuses in Hong Kong SAR, China and Singapore.
In order to provide more solid evidence for the effects of vaccination coverage, we further collected data from 52 Omicron variant dominated countries/regions and conducted multiple linear regressions. After adjusting for GDP per capita, proportion of people aged 70 and older, population density, hospital beds per 1,000 people, human development index, and cardiovascular mortality per 100,000 people, we found that a higher coverage of ≥1 dose vaccination, full vaccination, and booster vaccination were all negatively associated with lower CFRs (
Supplementary Table S2 ). Moreover, full vaccination and ≥1 dose vaccination coverages were the top two contributing factors to CFR (Figure 1).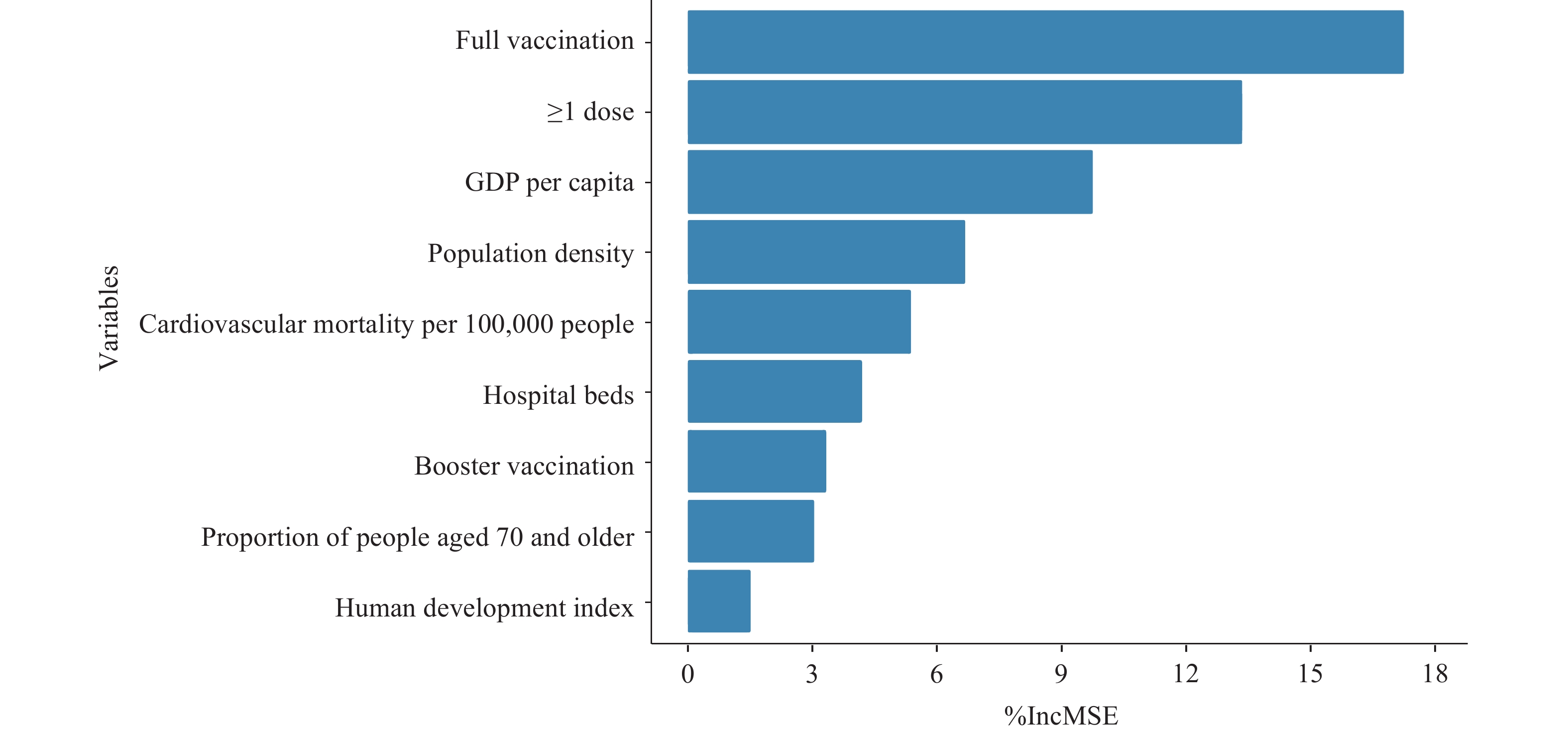 Figure 1.
Figure 1.The importance rank of contribution variables to CFR using a RF model.
Note: Full vaccination refers to people who received all doses prescribed by the initial vaccination protocol (commonly 2 doses and sometimes 3 doses, depending on the definition by the corresponding countries) per 100 people in the total population of the country or region; ≥1 dose refers to people who received at least 1 dose vaccination per 100 people in the total population of the country or region.
Booster vaccination refers to people with doses administered beyond the number prescribed by the initial vaccination protocol (commonly 3 doses and sometimes 4 doses, depending on the definition by the corresponding countries or regions) per 100 people in the total population of the country or region.
The detailed information of other variables is presented in
Supplementary Table S1 .Abbreviation: CFR=case fatality ratio; RF=random forest regression model; %IncMSE=percentage increase in mean square error.
-
The CFR in Hong Kong SAR, China during the 5th wave of COVID-19 is much higher than in Singapore, which could be attributed to the relatively low vaccination coverage, especially in elderly populations in Hong Kong SAR, China.
A systematic review indicated that age was the strongest predictor of infection–fatality ratio (IFR) during the pre-vaccine period (7). The age-specific IFR during the pre-vaccine period formed a J shape. A series of reasons, like immunosenescence, underlying diseases, and age-related damage could explain the higher IFR in the elderly (7–8). Fortunately, vaccination, especially booster vaccination, has been proved effective in reducing COVID-19 related deaths for the elderly (9). We also observed that the CFRs in fully vaccinated and booster vaccinated people were lower than in non-fully vaccinated people in Hong Kong SAR, China and Singapore. This difference should also be interpreted with the consideration of the “healthy vaccinee effect.” That is people with better health conditions are more likely to adhere to recommended vaccination, which may underestimate the CFR of vaccinated people.
In this study, after adjusting for confounding variables in the countries with a proportion of Omicron variant more than 90%, we also observed that ≥1 dose, full vaccination, and booster vaccination were all effective at reducing CFR. Unexpectedly, the effect and the importance of boosters were lower than the other two vaccination statuses, which may be explained by the low booster vaccine coverage in elderly populations. After the initial booster vaccination, young people could have lower vaccination hesitancy than the older adults and comprise a larger proportion of people vaccinated with a booster dose. Together with the lower mortality risk of young people, the real effect of booster vaccine coverage (normally higher than the coverage of full vaccination) will not emerge until more people, especially older adults, receive booster vaccines. In addition, a large observational study in Hong Kong SAR, China indicated that receiving two doses of mRNA vaccine (vaccine effectiveness: 89.3%) and inactivated vaccine (vaccine effectiveness: 69.9%) could all achieve good effectiveness against COVID-19 related severe diseases and deaths in the elderly (10). This study also indicated that receiving three doses of both mRNA and inactivated vaccine could offer superior effectiveness than two doses (10). The real-world evidence in Hong Kong SAR, China indicates that the elderly should get any type of accessible vaccine whenever possible.
Outside of vaccination status, the following factors may contribute to a higher CFR in Hong Kong SAR, China than in Singapore. First, Hong Kong SAR, China has a higher proportion of people aged 70 and older (12.10%) than Singapore (7.30%) (
Supplementary Figure S1 ). Second, the prevalence of chronic diseases in Hong Kong SAR, China is higher than in Singapore (Supplementary Table S3 ). The prevalence of obesity is 29.9% in Hong Kong SAR, China and only 8.7% in Singapore. The prevalence of hyperlipidaemia and hypertension is also higher in Hong Kong SAR, China than in Singapore (hyperlipidaemia: 49.5% vs. 33.6%, hypertension: 27.7% vs. 21.5%). Third, in Singapore, a total of 279,450 cases of COVID-19 have been reported as of December 31, 2021. On the contrary, Hong Kong SAR, China has only 12,649 reported cases before 2022, which makes the infection rate in Hong Kong SAR, China (0.20%) before 2022 is lower than that in Singapore (4.80%). Fourth, the number of COVID-19 infections was higher in Singapore than in Hong Kong SAR, China before late February, but the proportion of hospital beds occupied by COVID-19 patients was higher in Hong Kong SAR, China than in Singapore since mid-February (Supplementary Figure S2 ), which could be attributed to the imperfect tiered diagnosis and treatment strategy during the early Omicron epidemic in Hong Kong SAR, China. A few patients without severe symptoms occupied hospital beds, which led to an overwhelmed medical system unable to treat patients with severe illness and contributed to a higher CFR. Finally, the average daily number of swab tests (including polymerase chain reaction and rapid antigen test) of COVID-19 in Hong Kong SAR, China was 22.5 tests per 1,000 people (January to March 2022), while in Singapore it was 37.8 tests per 1,000 people (December 31, 2021 to March 14, 2022) (Supplementary Table S4 ). In conclusion, this comparison between Hong Kong SAR, China and Singapore indicates that vaccination has had good efficacy in preventing deaths from COVID-19. This real-world evidence calls on non-vaccinated, non-fully-vaccinated and non-booster-vaccinated people, especially the elderly, to get any type of accessible vaccine, which could save lives.
HTML
| Citation: |

|