
 Download:
Download:




-
At the beginning of April 2019, China National Health Commission (NHC) and China Center for Disease Control and Prevention (China CDC) received reports of a cluster of febrile illness involving about ten Chinese workers in a manganese ore in Cooperative Republic of Guyana. The enterprise applied to NHC for permission for evacuating the patients back to China for further treatment. A special Chinese medical team composed of the experts of epidemiology, medical bacteriology, clinical and emergency medicines was deployed to Georgetown, Guyana on April 6, 2019 to provide the support in clinical and public health, to identify the potential etiology and to assess the potential threat, especially the risk of international transmission.
HTML
-
On March 28, 2019, six Chinese males with fever visited the local Pakera District Hospital (PDH) in Matthews Ridge. They complained of non-productive coughing, headaches, weakness and joint pain, and two of them had severe symptoms. All of them came from a manganese ore mine nearby. After hospitalization, the District Medical Officer (DMO) notified this event to the Chief Medical Officer (CMO) of the Ministry of Public Health (MOPH) of Guyana immediately and MOPH operationalized its emergency responses operations quickly. One day later, a patient’s condition suddenly deteriorated and died with a manifestation of hemorrhagic and multi-organ failure. The rest of the five patients were further transferred to Georgetown Public Hospital (GPH) on March 30, 2019. In the following days, eight more cases including seven Chinese workers and one Guyanese worker were successfully identified and transferred to GPH. Two other mild cases with only mild fever stayed in PDH. Another severe patient displayed multi-organ failure and died in GPH on April 3, 2019.
Based on the signs and symptoms of the six patients, the MOPH of Guyana issued a working case searching definition: a person who had fever, with or without any one of the below symptoms with unexplained reasons such as cough, headaches, weakness, muscle, and/or joint pains since March 1, 2019 in Matthews Ridge. Healthy miners in the manganese ore mine who had entered the same abandoned tunnels and the close contacts of the patients were placed under medical observation. Up to April 15, 2019, a total of 16 patients were identified. Two Chinese patients died, and two cases (one Chinese patient and one Guyanese patient) were discharged. Because the Guyanese patient showed negative laboratory test results and had no exposure to the abandoned mines, he was excluded from the final case-list. A total of 24 miners including 10 healthy co-exposed miners and 14 close contacts were under medical observations in Matthews Ridge.
-
Various tissue specimens from the two fatal cases and blood samples from surviving patients were transferred to the laboratories of China CDC. Next-generation sequencing (NGS) technology based on Illumina MiSeq platform identified different lengths of specific gene sequences of Histoplasma capsulatum in seven different samples of two fatal cases and one severe case, including lung and blood samples. Up to April 15, 7 cases were laboratory confirmed as being infected with Histoplasma capsulatum. Therefore, 7 of 15 patients were laboratory confirmed cases and the remaining 8 patients were clinically diagnosed cases (Table 1).
Case No. Age (years) Date of Onset Type of diagnosis Clinical Outcome Clinical evaluation score† Details of exposure in the four old mines Date of first entry Date of last entry Times of entry No. of mines Type of work Place of work Hours of stay per time Other miner's working§ Exposure intensity¶ 1 47 Mar 22 Laboratory confirmed Dead 100 Mar 16 Mar 22 7 4 Shovel Bottom 2 Yes 189 2 44 Mar 26 Laboratory confirmed Dead 100 Mar 16 Mar 25 7 4 Shovel Bottom 2 Yes 270 3 42 Mar 27 Laboratory confirmed Coma, ICU 90 Mar 16 Mar 27 5 4 Shovel, crush Bottom, middle 2 Yes 175 4 51 Mar 25 Laboratory confirmed ICU 90 Mar 17 Mar 23 5 4 Shovel Bottom 2 Yes 171 5 49 Mar 29 Laboratory confirmed Hospitalization 70 Mar 16 Mar 27 7 4 Shovel, crush Bottom, middle 2 Yes 249 6 33 Mar 29 Clinical diagnosis Hospitalization 1 Mar 18 Mar 18 1 1 Check around Bottom 0.1 Yes 0.113 7 44 Mar 28 Laboratory confirmed Hospitalization 1 Mar 24 Mar 27 4 4 Crush, check around Bottom 1.5 No 9.6 8 56 Mar 30 Clinical diagnosis Hospitalization 20 Mar 16 Mar 24 2 4 Check around Bottom 0.1 No 0.525 9 34 Mar 30 Clinical diagnosis Hospitalization 30 Mar 18 Mar 28 1 2 Crush Bottom 1.5 Yes 5.625 10 48 Mar 30 Clinical diagnosis Hospitalization 1 Mar 16 Mar 16 2 1 Check around Bottom 0.1 Yes 0.225 11 43 Mar 30 Clinical diagnosis Hospitalization 5 Mar 17 Mar 27 1 2 Check around Bottom 0.1 Yes 0.3 12 38 Mar 31 Clinical diagnosis Discharge 0.5 Mar 16 Mar 16 1 1 Check around Entrance 0.5 No 0.094 13 50 Mar 26 Laboratory confirmed ICU 80 Mar 16 Mar 24 7 4 Shovel Bottom, middle 2 Yes 198 14 41 Apr 11 Clinical diagnosis Hospitalization 30 Mar 28 Mar 28 1 1 Crush Middle 1.5 Yes 2.25 15 23 Apr 11 Clinical diagnosis Hospitalization 30 Mar 28 Mar 29 2 2 Crush Entrance 6 Yes 12 Abbreviation: ICU = intensive care unit. All 15 cases were male. Next-generation sequencing (NGS) technology based on Illumina MiSeq platform identified different lengths of specific gene sequences of Histoplasma capsulatum in 7 different samples of 2 fatal cases and one severe case, including lung and blood samples. Up to April 15, 2019, 7 cases were laboratory confirmed being infected with Histoplasma capsulatum.
* All data were updated as of April 15, 2019 when the special Chinese medical team departed from Guyana back to China.† A clinical evaluation score (range: 0.5 to 100) was assigned to each of the 15 Chinese cases by clinical experts according to their illness severity. The more severe the illness was, the higher score was. § Were other miners working close by? ¶ The exposure intensity was a score representing the exposure degree and risk of infection according to the detailed exposure information of the case-patients. It was calculated by using the equation of $\sum\nolimits_{F = 1}^n {\left( {{{twTLE}}} \right)} $; n was the number of the abandoned tunnels (range: 1-4), F was the times of entry, t was hours of stay per entry, w was the type of work including shovel (score=1.5), crush (score=1) and inspection (score=0.5), T was the date of entry including Period 1 (score=1.5) from March 13 to 22, 2019 and Period 2 (score=1) from March 23 to 29, 2019, L was the place of work including the bottom (score=1.5), middle (score=1) and entrance (score=0.5) of the tunnels, and E indicated whether other work was performed during the stay (Yes scoring 1, No scoring 0.5).Table 1. The epidemiological and clinical characteristics of the 15 Chinese manganese-miner male case-patients in the outbreak of febrile illness in Matthews Ridge, Cooperative Republic of Guyana in 2019*
-
The investigation was conducted by carefully interviewing the patients and their healthy co-workers. The median age of 15 Chinese male patients was 43.5 years old (range: 23-56). The first case displayed clinical manifestation on March 22, 2019 and the peak of disease was on March 30, 2019 (Table 1 and Figure 1). Fever was the most frequent symptom (n=15, 100%), while other symptoms were also noticed including headache (n=10, 67%), muscle pains (n=8, 53%), joint pains (n=8, 53%), weakness (n=7, 47%), cough (n=3, 20%), skin rash (n=3, 20%), and dizziness (n=1, 7%). A clinical evaluation score (range: 0.5 to 100) was assigned to each of the 15 Chinese cases by clinical experts according to illness severity. The more severe the illness was, the higher score was assessed. Among the 15 cases, 2 were fatal cases, 4 were severe cases, and 9 were milder cases (Table 1). The median incubation period of all 15 cases was estimated as 10 days (range 2-11.5 days). The median incubation period of 6 severe and fatal cases [4 days (range 1.5-10 days)] was estimated significantly higher than that of 9 milder cases [12.5 days (range 8.5-13.5 days)].
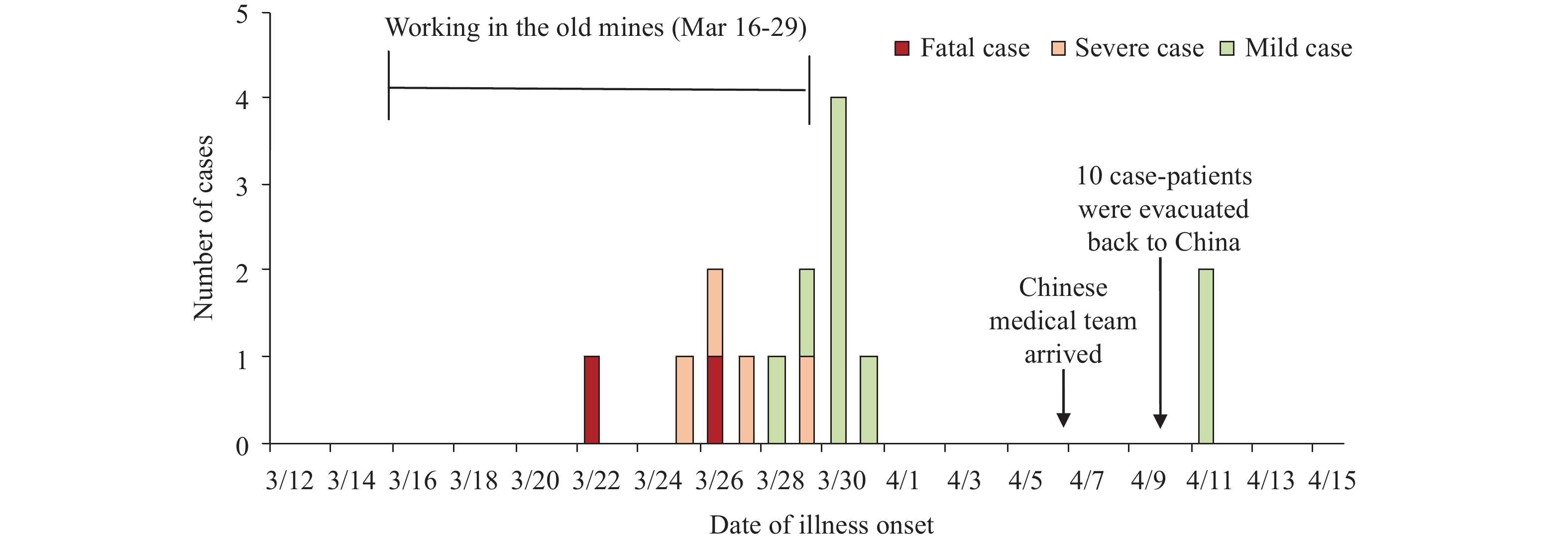 Figure 1.
Figure 1.The date of illness onset of the Chinese-manganese-miner male case-patients in the outbreak of febrile illness in Matthews Ridge, Cooperative Republic of Guyana in 2019
It was found that all 15 Chinese patients worked in 4 short tunnels (less than 20 meters long) during March 16 and 29, 2019, with varying labor hours. The tunnels were abandoned for more than 50 years. Bats were observed to live inside, and the feces of bats were observed on the ground during the field investigation. The workers entered the tunnels for waste clearance, including shoveling soil and crushing the concrete of the ground without any PPE. Neither the 10 co-workers who had also entered in those tunnels nor the 14 close contacts got sick, resulting an attack rate of 38.5%, and the exposure’s odds ratio (OR) of 2.4 (1.495-3.853) (p<0.0001). This strongly highlights that all patients in this event were exposed to the same pathological agent, and the possibility of human-to-human transmission is extremely limited.
-
As shown in Table 1, the frequency of entry and duration of stay inside of the tunnels among the 15 Chinese patients varied largely. To evaluate the exposure intensity of cases, an equation was used as below:
$$\mathop \sum \nolimits_{F = 1}^n \left( {{{twTLE}}} \right)$$ Of note, n was the number of abandoned tunnels (range: 1-4), F was the times of entry, t was hours of stay per entry, w was the type of work including shovel (score=1.5), crush (score=1), and inspection (score=0.5), T was the date of entry including Period 1 (score=1.5) from March 13 to 22 and Period 2 (score=1) from March 23 to 29, L was the place of work including the bottom (score=1.5), middle (score=1) and entrance (score=0.5) of the tunnels, and E indicated whether other work was performed during the stay (Yes scoring 1, No scoring 0.5).
Two distinct profiles of exposure intensity among the patients were clearly noticed. One was above 170 and the other was below 15. A logistic regression model [y=11.882ln(x)+18.405] was established by combining the exposure intensity scores of the cases with the individual clinical scores. The distribution of the 15 patients were distinctly divided in two separate areas (Figure 2). Patients with severe clinical manifestations and poor prognosis harbored significantly higher exposure intensity scores, in which 2 fatal cases showed exposure intensity scores of 189 and 270. Patients with low exposure intensity scores underwent mild clinical processes (Table 1). These data indicate a close relationship between the exposure intensity and disease severity.
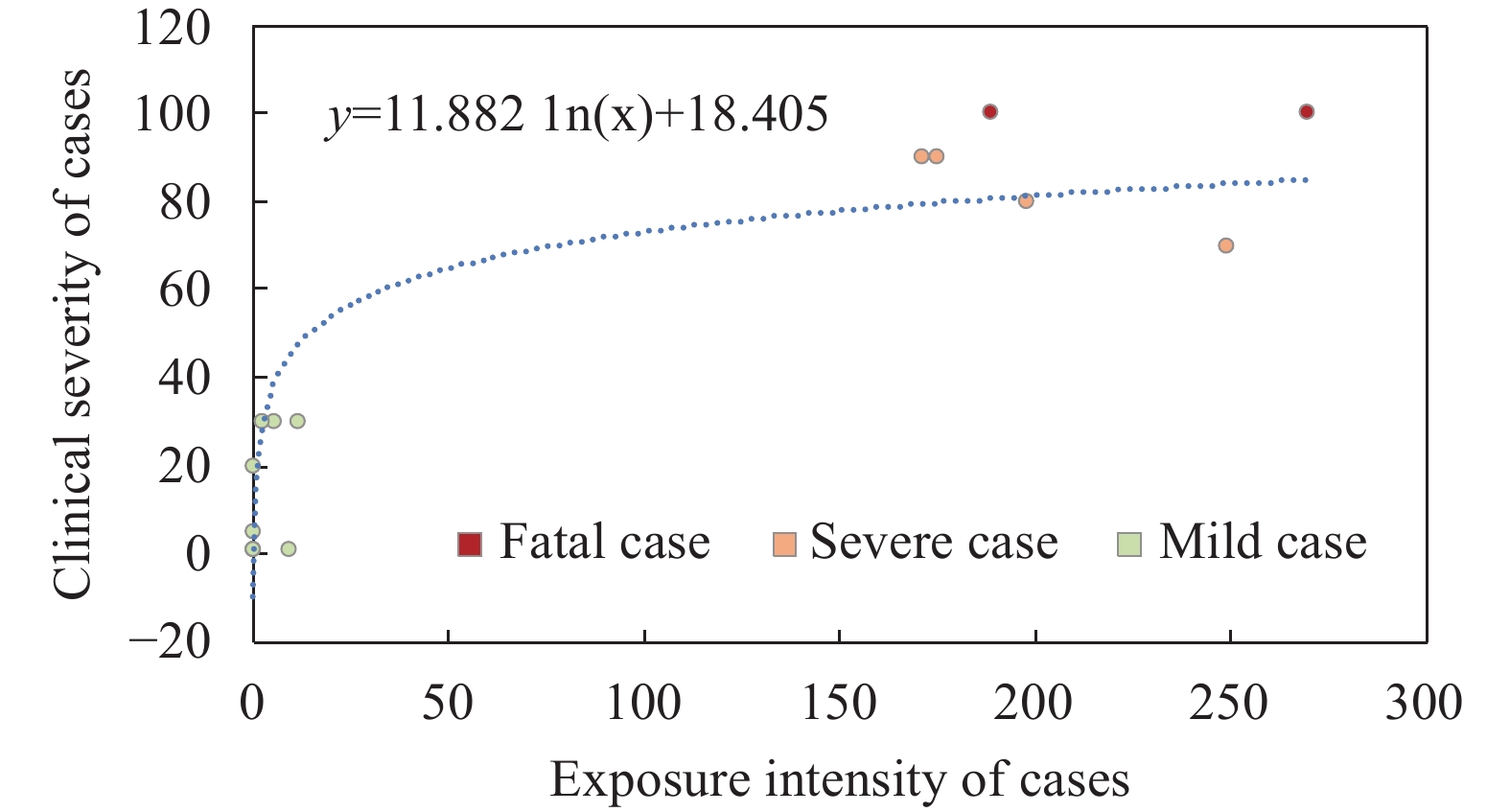 Figure 2.
Figure 2.The dose-response exposures associated with severity of illness among 15 Chinese-manganese-miner male case-patients in the outbreak of febrile illness in Matthews Ridge, Cooperative Republic of Guyana in 2019

-
In this overseas investigation among Chinese workers, a closely dose-dependent association of illness onset and disease severity with the exposure intensity to soil and waste possibly contaminated by the Histoplasma has been proposed. Long labor times, repeated entering of contaminated tunnels, working in dustier environments are likely to result in earlier illness onsets, more severe clinical courses and even fatal outcomes. More importantly, none of the patients used reliable PPE, such as common masks while working, that would prevent the inhalation of more Histoplasma spores. Finally, ten patients were successfully evacuated from Guyana to China with a Chinese medical aid aircraft without causing any further transmission. This outbreak practiced and exercised the Chinese medical emergency response overseas, but this investigation was limited because the environmental risk of the mines could not be evaluated. Environmental specimens collected in the mines were not been shipped to China on time due to restricted cooperation on specimen transportation between the countries.
The infection of Histoplasma has been reported in some countries in Southern America(1-2), including Guyana(3). During an interview with the staff in the local hospital, we learned that there was a local farmer who underwent similar but mild pathogenesis after entering the same tunnels and collecting feces of bats as fertilizer, highlighting the possibility of a long-term circulation of Histoplasma in this region. Although the clinical features of this cluster disease are similar to that of acute infections of Histoplasma described elsewhere(4-7), such a cluster outbreak is fairly rare in China. To our knowledge, no definitively confirmed cluster infection of Histoplasma in China has been reported. Despite that, there have been a few similar events that occurred in travelers in the caves in the southwestern region of China, inhabited various species of bats, though no reliable pathogen evidence has been obtained. The clinical findings of the cases provide valuable experience to Chinese clinicians to understand the clinical features of acute infection of Histoplasma and will help achieve early detection and efficient treatment for patients. Although information on the miners’ reference level of health is not available for further comparative analysis, the epidemiological findings of this outbreak investigation highlight a probable risk of infection with Histoplasma when entering without PPE into environments inhabited by bats such as caves or mines. Education and communication initiatives might benefit residents and travelers in this region. This outbreak expands our knowledge of the control and prevention of fungal disease in China. Due to worldwide industrial collaborations and traveling, we to need watch closely for emerging pathogens(8).
-
All authors have no reported conflicts. We thank Dr. Shamdeo Persaud, the Chief Medical Officer (CMO) and other staff of the Ministry of Public Health (MOPH) of Guyana, the staff in Pakera District Hospital (PDH) in Matthews Ridge and Georgetown Public Hospital (GPH) in Guyana for the support and assistance during the field investigation. We thank the staff members from Chongqing Health Commission and Chongqing CDC, and physicians from Beijing 999 Emergency Center for their support of field investigations and data collection. We also thank the staff of the National Institute for Communicable Disease Control and Prevention, and the staff of the Institute for Viral Disease Control and Prevention in China CDC for IV technical support in laboratory testing. We appreciate Dr. Chin-kei Lee for his comments and suggestions.
This work was supported by the Ministry of Science and Technology of China, Emergency Technology Research Issue on Prevention and Control for Human Infection with A(H7N9) Avian Influenza Virus [KJYJ-2013-01-02], the China-US Collaborative Program on Emerging and Re-Emerging Infectious Disease, and National Mega-Projects for Infectious Disease [2018ZX10201002-008-002], and the National Natural Science Foundation (NSFC, 71934002).
| Citation: |

|