
 Download:
Download:




-
Nocardia species are found worldwide in soil rich in organic matter (1). As of April 2025, 252 Nocardia species have been identified, and approximately 50 of them are considered human pathogens (https://www.bacterio.net/) (2–3). Most Nocardia infections are acquired through inhalation or traumatic inoculation (4–7). Infections are often seen in immunocompromised hosts, such as patients with AIDS, autoimmune diseases, malignancies, diabetes mellitus, or organ transplants (8–10). Infection with Mycobacterium tuberculosis (TB) is associated with chronic lung disease, and the similarity in the diagnosis and clinical manifestations of nocardiosis and TB may lead to misdiagnosis (11). The treatment of choice for tuberculosis is ineffective against nocardiosis, underscoring the importance of accurate diagnosis for effective therapy. The antimicrobial susceptibility of Nocardia is highly variable and depends on the species. Several studies have raised concerns about increasing resistance among Nocardia isolates, particularly to trimethoprim-sulfamethoxazole (SXT). Similarly, breakthrough infections have been reported in immunocompromised individuals receiving SXT prophylaxis (12).
The present study is an extension of a previous investigation (13), focusing on 63 clinical Nocardia isolates collected from 11 provincial-level administrative divisions (PLADs) across 6 of the 7 administrative regions of China. Variability in antimicrobial susceptibility was observed among isolates of the same species. Overall, this study highlights the need for better assessment of the burden of nocardiosis in China and for continuous monitoring of antimicrobial resistance among Nocardia isolates.
-
We collected 305 clinical samples, 63 of which were identified as Nocardia strains. These isolates were obtained from patients across 11 PLADs in China, representing 6 of the 7 administrative regions. Phylogenetic analysis of the 16S rRNA gene was conducted to determine the species. Antimicrobial susceptibility to 32 antibiotics was determined using the broth microdilution method in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines (14). The Alamar Blue assay was used as the visual endpoint indicator, as previously described (13). The minimum inhibitory concentration (MIC) was defined as the lowest drug concentration that inhibited visible growth of the tested isolates. Cluster analyses of samples and antibiotics were performed using SPSS Statistics (version 22.0; IBM, Armonk, New York, USA), and both antibiotic and sample clusters were analyzed through hierarchical cluster analysis.
-
The sample sources were diverse, including eye secretions, sputum, abscesses, blood, bronchoalveolar lavage fluid, cerebrospinal fluid, and lung or liver biopsies. The most represented species was N. farcinica (23; 36.5%), followed by N. cyriacigeorgica (17; 27.0%). Three species were marginally represented in the dataset: N. brasiliensis (6; 9.5%), N. otitidiscaviarum (5; 7.9%), and N. beijingensis (4; 6.3%). Four species were rarely represented: N. asiatica, N. terpenica, N. veterana, and N. abscessus (
Supplementary Table S1 ). One sequence (159) showed 98.4% identity with N. nova based on BLASTn analysis, while two sequences (153 and 160) did not match any of the established Nocardia species (Supplementary Figure S1 ). -
MIC values were determined for 32 antibiotics from 13 drug classes, with β-lactam antibiotics (9 drugs) (Figure 1). The resulting heatmap was analyzed in two ways: based on MIC values themselves and based on breakpoint values determined for each antibiotic by CLSI. To identify trends between strains and antibiotics, cluster analysis was performed on both the strains and the drugs (Figure 1). As mentioned earlier, phylogenetic analysis of the 16S rRNA gene identified 10 groups –– nine corresponding to known species and one containing the two undetermined sequences, 153 and 160. A cluster analysis was performed using 12 clusters, considering that strains 153 and 160 were genetically distinct. Overall, the cluster analysis did not correspond to species determination. For example, the 23 N. farcinica strains were distributed across six clusters, with cluster 1 containing 17 of these strains. The six remaining strains (170, 158, 178, 165, 176, and 335) showed significantly different MIC patterns. Strain 170 in cluster 4 and strains 158 and 178 in cluster 2 exhibited strong resistance to cefotaxime (CTX) (MIC 256 mg/L) compared with other N. farcinica strains. Strain 165 in cluster 5 showed an intermediate MIC value for isoniazid (INH) (8 mg/L). Strain 176 in cluster 3 showed strong resistance to gentamicin (GEN) (MIC 256 mg/L). Finally, strain 335 in cluster 6 showed strong resistance to cefmetazole (CMZ), ceftriaxone (CRO), cefotaxime (CTX), cefoxitin (FOX), ethambutol (ETH), streptomycin (STR), clofazimine (CLO), and kanamycin (KAN) (256 mg/L). A discrepancy between species determination and cluster analysis was observed for all species except N. brasiliensis and N. asiatica, which were found in clusters 1 and 7, respectively. N. cyriacigeorgica strains were found in clusters 1 and 4, N. otitidiscaviarum in clusters 11 and 12, and N. beijingensis in clusters 1 and 7, respectively. The 63 strains showed intermediate MIC values for clindamycin (CLI) (8–64 mg/L). All strains except one (165) showed high MIC values for INH (256 mg/L). Although the strains were initially divided into 12 clusters, these clusters could be grouped into two mega groups: A (clusters 1–5 and 7) and B (clusters 6 and 8–12). The main difference between these two mega groups involved CMZ, with group A showing a lower average MIC (27.1 mg/L) and group B showing a higher average MIC (243.2 mg/L). In group A, cluster 7 was characterized by high ciprofloxacin (CIP) and levofloxacin (LVX) (128–256 mg/L), whereas cluster 3 was characterized by high GEN (256 mg/L). In group B, cluster 6 was characterized by high GEN values (32–256 mg/L) compared with other strains in group B (average, 0.8 mg/L).
 Figure 1.
Figure 1.Heatmap showing MIC values of 63 Nocardia clinical isolates for 32 antimicrobial drugs.
Note: Drugs used to treat TB are shown in red font. Isolate species were determined by phylogenetic analysis of the 16S rRNA gene. MIC data were clustered by strains as well as drugs. Trees based on cluster analyses are shown on the right for the strains and at the top for the drugs. In both cases, 12 clusters were identified and are color-coded and numbered. Drug classes are indicated by a number. MIC values were also color-coded, from blue (MIC of 0.125 mg/L) for a susceptible strain to red (MIC of 256 mg/L) for a resistant strain. Clusters based on the strains were organized into two mega groups, labeled A and B. Similarly, clusters based on drugs were organized into two mega groups, labeled I and II. The average MIC value for each drug is shown at the bottom and is color-coded. Breakpoint values for each drug are also shown at the bottom. Average MIC values below the breakpoint are highlighted in green.
Abbreviation: MIC=minimum inhibitory concentration; TB=tuberculosis; AMK=amikacin; AMC=amoxicillin-clavulanate; AMP=ampicillin; AZM=azithromycin; FEP=cefepime; CMZ=cefmetazole; CTX=cefotaxime; FOX=cefoxitin; CRO=ceftriaxone; CIP=ciprofloxacin; CLR=clarithromycin; CLI=clindamycin; CLO=clofazimine; DOX=doxycycline; ETH=ethambutol.
Cluster analysis was performed based on the drugs. The 32 drugs belonged to 13 drug classes. The most represented class was β-lactam antibiotics, comprising nine drugs that were distributed across three different clusters (1, 2 and 3). Five of these drugs were found in cluster 1. The drugs were further grouped into two mega groups, I and II, with three clusters (clusters 6–8) forming the mega group II. Overall, group I showed low MIC values, whereas group II was characterized by high MIC values and included INH, RIF, and VAN. The clusters differed in their overall MIC values, with cluster 1 showing the lowest and cluster 7 the highest.
The average MIC value was calculated for each drug across all 63 clinical samples. Three antibiotics (linezolid, amikacin, and meropenem) had mean MIC values below their respective breakpoints, suggesting that these antibiotics were likely effective against all clinical isolates analyzed. However, variations were observed both between and within species. For example, N. otidiscavarium strains 155 and 324 had intermediate MIC values for tobramycin (TOB) (8–64 mg/L), whereas the other three N. otidiscavarium strains had MIC values below the TOB breakpoint value (4 mg/L). Three antibiotics — minocycline (MIN), doxycycline (DOX), and moxifloxacin (MXF) — had average MIC values (2.6, 3.8, and 3.8 mg/L, respectively) that were close to their breakpoint values (1 mg/L for all three) and might also be considered effective against most Nocardia species.
-
The previous analysis did not reveal any significant trend in antibiotic resistance across species. The next step was to assess whether any resistance pattern was consistent among all clinical strains of the same species. Although nine species were reported in this study, only five were analyzed because the remaining species were represented by only one or two clinical strains. Only the drugs for which MIC values exceeded the breakpoint value for each clinical isolate are listed in Table 1. Six resistance patterns were identified among the antibiotics and Nocardia species. Lincosamides (CLI) and INH were ineffective against all clinical isolates of the five Nocardia species. Six additional drug classes –– ETH, ansamycin (rifampin, RIF), glycopeptides (vancomycin), tetracyclines (tigecycline), phenazine (clofazimine), and sulfonamides (sulfamethoxazole) –– were ineffective against at least two species. Among macrolides, clarithromycin (CLR) was ineffective against all five species, whereas azithromycin (AZM) was ineffective against four of the five analyzed species. The effectiveness of β-lactams and fluoroquinolones varied by both drug and species. GEN was ineffective against N. farcinica, whereas KAN and STR were ineffective against two species. The last category concerned oxazolidinone (linezolid, LZD), which is not listed in Table 1, indicating that this drug might be effective against at least one clinical isolate from each of the five analyzed species. Consistent susceptibility to both amikacin (AMK) and LZD was observed across all five Nocardia species, while complete resistance was observed against CLR, CLI, and INH (Tables 2–3). Overall, this analysis demonstrated that Nocardia species can exhibit variable responses to different antibiotics.
Antibiotic class Species† Category N. farcinica (23) N. cyriacigeorgica (17) N. brasiliensis (6) N. otitidiscaviarum (5) N. beijingensis (4) Lincosamides (1)* CLI § CLI CLI CLI CLI 1 Isoniazid (1) INH INH INH INH INH 1 Ethambutol (1) ETH ETH ETH ETH 2 Ansamycin (1) RIF RIF RIF RIF 2 Glycopeptide (1) VAN VAN VAN 2 Tetracyclines (3) TGC TGC 2 Sulfonamides (2) SMZ SMZ 2 Phenazine (1) CLO CLO 2 Macrolides (2) CLR CLR, AZM CLR, AZM CLR, AZM CLR, AZM 3 β-lactams (9) FOX FOX, CMZ, IPM AMP, AMC, FEP, CTX,
FOX, CMZ, CRO, IPMAMC 4 Fluoroquinolones (4) CIP, LVX, OFX LVX, OFX CIP, LVX, OFX CIP, LVX, OFX 4 Aminoglycosides (5) GEN, KAN KAN, STR STR 5 Oxazolidinone (1) 6 Abbreviation: AMK=amikacin; AMC=amoxicillin-clavulanate; AMP=ampicillin; AZM=azithromycin; FEP=cefepime; CMZ=cefmetazole; CTX=cefotaxime; FOX=cefoxitin; CRO=ceftriaxone; CIP=ciprofloxacin; CLR=clarithromycin; CLI=clindamycin; CLO=clofazimine; DOX=doxycycline; ETH=ethambutol; GEN=gentamicin; IPM=imipenem; INH=isoniazid; KAN=kanamycin; LVX=levofloxacin; LZD=linezolid; MEM=meropenem; MIN=minocycline; MXF=moxifloxacin; OFX=ofloxacin; RIF=rifampicin; STR=streptomycin; SMZ=sulfamethoxazole; TGC=tigecycline; TOB=tobramycin; SXT=trimethoprim-sulfamethoxazole; VAN=vancomycin.
* Antibiotic classes were sorted based on the category column. The number of drugs in each class is indicated in parentheses.
† The number of clinical isolates for each species is indicated in parentheses.
§ Only drugs that were ineffective, i.e., with MIC values greater than breakpoint values for all clinical isolates of the analyzed species, are listed.Table 1. List of antibiotics ineffective against all clinical isolates of the five Nocardia species.
Species* Category Antibiotic Name Class
N. farcinica,
N. otitidiscaviarumAntibiotics effective on all clinical and reference strains AMK
LZDAminoglycoside
OxazolidinoneAntibiotics effective on all reference strains MXF
SXTFluoroquinolone
Sulfonamide
N. farcinicaAntibiotics effective on all clinical and reference strains AMC, IPM β-lactam Antibiotics effective on all reference strains MEM β-lactam
N. otitidiscaviarumAntibiotics effective on all clinical and reference strains GEN Aminoglycoside Antibiotics effective on all clinical strains KAN Aminoglycoside * Only two Nocardia species were analyzed, as the remaining species were represented by fewer than four clinical or reference strains. Table 2. Antibiotic categories based on the effectiveness of clinical and reference strains of the same Nocardia species.
-
The present study identified different MIC patterns among strains of the same species as well as within the same antibiotic class. Comparison with the MIC patterns of Nocardia reference strains was necessary (Figure 2). The number of strains of each species with MIC values lower than or equal to the breakpoint value is shown for the 63 clinical strains (C) and the 26 reference strains (S). Some antibiotics had the same effect on all strains (clinical or/and reference) of the same species and are labeled as “100” in Figure 2. Only species with four or more strains (clinical or reference) were included in the comparison.
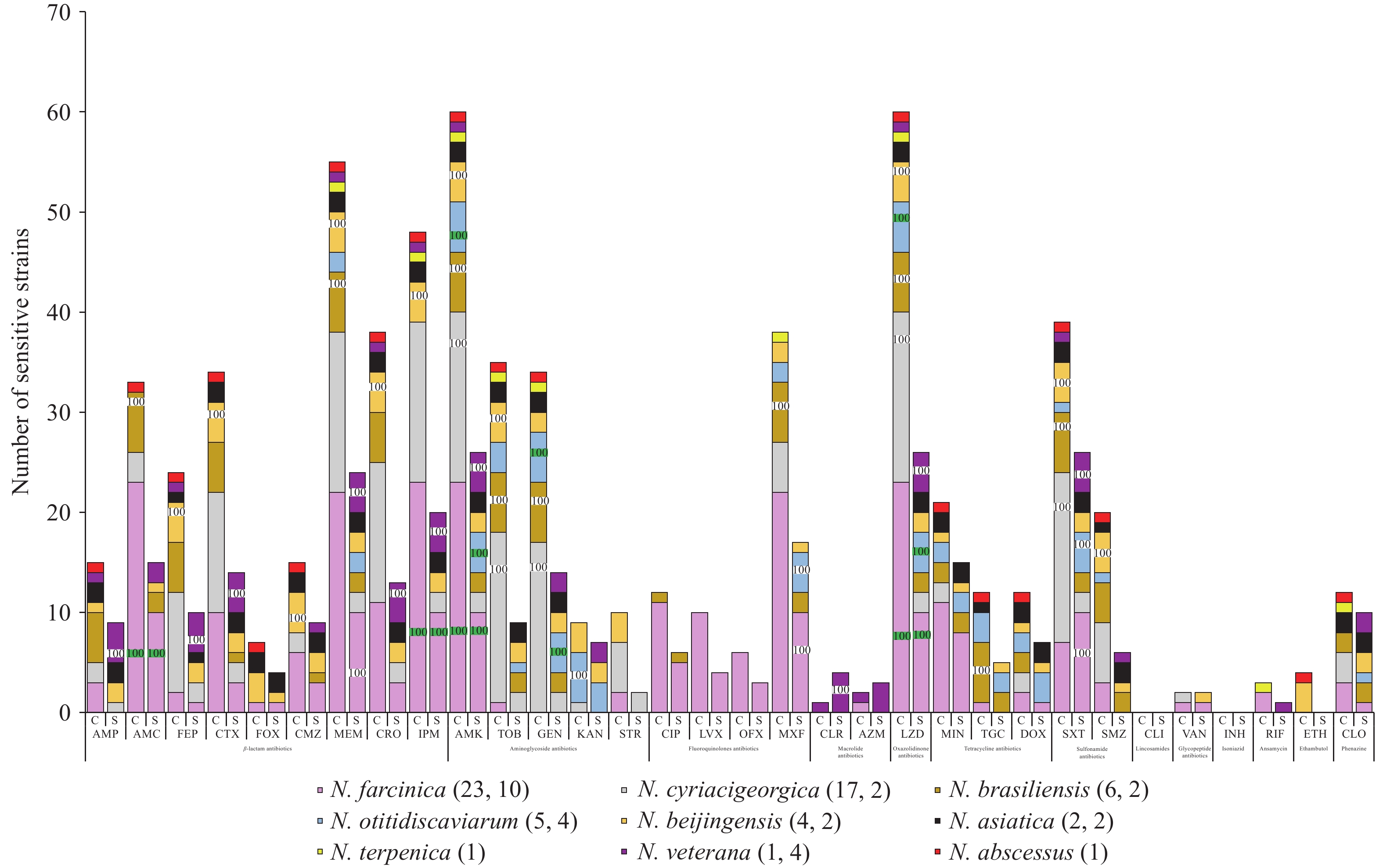 Figure 2.
Figure 2.Number of susceptible strains for each antibiotic.
Note: The number of strains with MIC values lower than the breakpoint value for each antibiotic is shown. Clinical (C) and reference (S) strains were analyzed. Species are color-coded according to the legend at the bottom. The number of clinical and reference strains is indicated in parentheses. Species for which all clinical and/or reference strains were susceptible to an antibiotic are labeled with “100”. Only species with four or more strains were included. Species for which all clinical and reference strains were susceptible to an antibiotic are shown with a green “100”, and the results are summarized in Table 2.
Abbreviation: AMK=amikacin; AMC=amoxicillin-clavulanate; AMP=ampicillin; AZM=azithromycin; FEP=cefepime; CMZ=cefmetazole; CTX=cefotaxime; FOX=cefoxitin; CRO=ceftriaxone; CIP=ciprofloxacin; CLR=clarithromycin; CLI=clindamycin; CLO=clofazimine; DOX=doxycycline; ETH=ethambutol; GEN=gentamicin; IPM=imipenem; INH=isoniazid; KAN=kanamycin; LVX=levofloxacin; LZD=linezolid; MEM=meropenem; MIN=minocycline; MXF=moxifloxacin; OFX=ofloxacin; RIF=rifampicin; STR=streptomycin; SMZ=sulfamethoxazole; TGC=tigecycline; TOB=tobramycin; SXT=trimethoprim-sulfamethoxazole; VAN=vancomycin; MIC=minimum inhibitory concentration.
Overall, four categories of antibiotics were identified based on their effectiveness in both clinical and reference strains (Table 2). First, AMK and LZD were effective against all clinical and reference strains of N. farcinica and N. otitidiscaviarum (labeled with “100” in green in Figure 2). Second, amoxicillin-clavulanate (AMC), imipenem (IPM), and GEN were effective against all clinical and reference strains of one species. AMC and IPM were effective against all the clinical and reference strains of N. farcinica, whereas GEN was effective against all the clinical and reference strains of N. otitidiscaviarum. Third, MXF, SXT, and meropenem (MEM) were effective against all 10 N. farcinica reference strains, whereas lower effectiveness was observed among the 23 N. farcinica clinical strains. Finally, KAN was effective against all five N. otitidiscaviarum clinical strains, whereas one N. otitidiscaviarum reference strain was highly resistant (MIC value 256 mg/L; breakpoint 4 mg/L). None of the drug classes used in this study were consistently effective against all clinical strains of the analyzed species. Among the seven TB drugs, resistance to INH was observed in the clinical strains of all analyzed species. GEN and KAN were the only drugs used to treat TB that showed some effectiveness against all Nocardia strains. Other TB drugs, including STR, RIF, ETH, and CLO, were effective against only a few Nocardia clinical strains (Table 3).
Antibiotic class* N. farcinica (23)† N. cyriacigeorgica (17) N. brasiliensis (6) N. otitidiscaviarum (5) N. beijingensis (4) β-lactams (9) FOX§ FOX, CMZ, IPM AMP, AMC, FEP, CTX, FOX, CMZ, CRO, IPM AMC AMP, FEP, CTX, FOX, CMZ, CRO, MEM AMP, AMC, FEP, CTX, CMZ, CRO, IPM, MEM AMP, FEP, CTX, CRO MEM AMP, FOX AMC, IPM AMC, MEM FEP, CTX, CMZ, MEM, CRO, IPM Aminoglycosides (5) GEN, KAN KAN, STR STR TOB, STR KAN, STR TOB GEN, KAN, STR AMK AMK, TOB, GEN AMK, TOB, GEN AMK, GEN, KAN AMK, TOB Fluoroquinolones (4) CIP, LVX, OFX LVX, OFX CIP, LVX, OFX, CIP, LVX, OFX, CIP, LVX, OFX, MXF, MXF, CIP, MXF MXF MXF Macrolides (2) CLR CLR, AZM CLR, AZM CLR, AZM CLR, AZM AZM Oxazolidinone (1) LZD LZD LZD LZD LZD Tetracyclines (3) TGC TGC MIN, TGC, DOX MIN, DOX MIN, DOX MIN, TGC, DOX MIN, DOX TGC Sulfonamides (2) SMZ SMZ SXT, SMZ SMZ SXT SXT SXT SXT, SMZ Phenazine (1) CLO CLO CLO CLO CLO Lincosamides (1) CLI CLI CLI CLI CLI Glycopeptide (1) VAN VAN VAN VAN VAN Isoniazid (1) INH INH INH INH INH Ansamycin (1) RIF RIF RIF RIF RIF Ethambutol (1) ETH ETH ETH ETH ETH Abbreviation: AMK=amikacin; AMC=amoxicillin-clavulanate; AMP=ampicillin; AZM=azithromycin; FEP=cefepime; CMZ=cefmetazole; CTX=cefotaxime; FOX=cefoxitin; CRO=ceftriaxone; CIP=ciprofloxacin; CLR=clarithromycin; CLI=clindamycin; CLO=clofazimine; DOX=doxycycline; ETH=ethambutol; GEN=gentamicin; IPM=imipenem; INH=isoniazid; KAN=kanamycin; LVX=levofloxacin; LZD=linezolid; MEM=meropenem; MIN=minocycline; MXF=moxifloxacin; OFX=ofloxacin; RIF=rifampicin; STR=streptomycin; SMZ=sulfamethoxazole; TGC=tigecycline; TOB=tobramycin; SXT=trimethoprim-sulfamethoxazole; VAN=vancomycin.
* The number of drugs in each class is indicated in parentheses.
† The number of clinical isolates for each species is indicated in parentheses.
§ Antimicrobial susceptibility of Nocardia species is color-coded as follows: red (resistant; MIC value greater than the breakpoint value for all clinical isolates of the analyzed species), blue (susceptible; MIC value less than or equal to the breakpoint value for all clinical isolates of the analyzed species), and yellow (intermediate).Table 3. Species-specific antimicrobial susceptibility of Nocardia strains.
-
The present study focused on the antibiotic susceptibility patterns of 63 clinical Nocardia strains collected in China. Recent studies identified N. farcinica and N. otitidiscaviarum as the most prevalent species, confirming the present findings (4,13,15). Although this study, which included 63 clinical isolates and nine known Nocardia species, extends a previous study that featured only 14 clinical isolates and three species, it is worth noting some limitations. Although clinical isolates from nine species were reported in the present study, only two species (N. farcinica and N. cyriacigeorgica) were represented by more than 10 strains. Another limitation concerned the number of reference strains for each species. Only three species ( N. farcinica, N. otitidiscaviarum, and N. veterana) were represented by four or more standard strains. Geographic distribution was also a limitation, as one administrative region –– Dongbei –– was not represented in the present study. The reported strains were collected from 11 PLADs with relatively developed economies in China. Despite these limitations, the present study identified important trends that should be further confirmed by additional research.
The present study identified antibiotics based on their efficiency against Nocardia species, revealing that two drugs, LZD and AMK, were effective against all analyzed N. farcinica, N. otitidiscaviarum species. These antibiotics were also effective against all analyzed strains in studies conducted in Henan and Shandong provinces (4,10,15). Our recent systematic review of antimicrobial susceptibility data from Nocardia clinical isolates in China (as of 2024) revealed relatively low overall resistance rates to three antibiotics: LZD (0.30%, 1/336), AMK (3.87%, 13/336), and SXT (3.87%, 13/336) (in press, Disease Surveillance).
The present study revealed differences in antibiotic susceptibility among the same Nocardia species. Strains of the same species were not all sensitive to the same antibiotics. Moreover, antibiotics belonging to the same drug class did not exhibit equal effectiveness against Nocardia strains. The most consistent drug class was the aminoglycosides, which showed some degree of effectiveness, with variations observed among Nocardia strains. A previous study reported similar findings, with AMK being effective against six of seven tested species (10).
In summary, the present study revealed potential genetic diversity among Nocardia strains, at least based on the 16S rRNA gene, which resulted in incomplete species identification. Moreover, differences in antibiotic susceptibility were observed among strains of the same species. Finally, a comprehensive analysis of Nocardia strains in China would be beneficial for monitoring the potential emergence of antibiotic resistance.
HTML
Antibiotic Resistance Patterns of the 63 Strains
Antibiotic Resistance in Five Species
Comparison with Nocardia Standards
| Citation: |

|