

 Download:
Download:




-
Depressive symptoms significantly affect the mental health of Chinese adolescents (1), with previous research indicating a prevalence rate of 24.3% (2). The presence of depressive symptoms in this demographic is particularly concerning due to its established association with several adverse outcomes. These include extensive and prolonged impairments in interpersonal relations, social interaction, educational achievement, and work performance (3). Moreover, depressive symptoms are linked to substance misuse and an increased risk of suicide (4). Although the precise causes of depression remain unclear, it is crucial to identify risk factors that are unique to adolescent depression to better prioritize intervention strategies. Bronfenbrenner’s ecological systems theory emphasizes that both individual characteristics and various environmental levels influence child and adolescent development (5). Despite previous studies investigating individual factors of adolescent depression, there remains a deficiency in comprehensive models that consider multidimensional influences and the interactions among different risk factors.
To thoroughly examine the factors influencing depressive symptoms in adolescents, identify the most significant ones, and delineate prevention targets, we conducted a cross-sectional study in eight secondary schools in Beijing. The study aimed to analyze the association between depressive symptoms and various factors such as personality, coping style, childhood abuse, school bullying, parent and peer attachment, and perceived stress among Chinese adolescents. Data collection occurred from July 7, 2022, to April 9, 2023, employing convenience sampling through a mix of online and field surveys. Rigorous data verification and quality control measures were implemented to ensure the integrity and accuracy of the data. Quality control personnel were assigned to verify the logic and completeness of the responses, achieving a questionnaire completion rate of 92.8% (1,671/1,800). The study protocol received approval from the Ethics Committee of Beijing Anding Hospital, and written informed consent was obtained from all participants and their parents.
We administered the 20-item Center for Epidemiologic Studies Depression Scale for Children (CES-DC), a self-report screening tool designed to assess depressive symptoms in adolescents. Scores exceeding 20 are indicative of depressive symptoms in the general population. On an individual level, personality and coping styles were evaluated. Personality was assessed using the Revised Eysenck Personality Questionnaire (EPQ-R), which measures four traits across 88 items: extraversion, neuroticism, psychoticism, and a lie scale, with higher scores suggesting a greater degree of the respective personality traits. Coping styles were assessed using the Simplified Coping Style Questionnaire (SCSQ), which consists of two dimensions: positive coping (12 items) and negative coping (8 items), where higher scores on each dimension indicate more pronounced coping strategies.
At the level of school and family environments, factors such as childhood abuse and neglect, parental and peer attachments, and peer victimization were considered. Childhood abuse and neglect were quantified using the Childhood Trauma Questionnaire-Short Form (CTQ-SF), which comprises 28 items across five dimensions: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. Higher scores on each dimension denote a higher level of reported abuse or neglect. Parental and peer attachments were assessed using the Inventory of Parent and Peer Attachment (IPPA), which measures the quality of attachments to fathers and mothers separately, focusing on key aspects of attachment such as trust, communication, and alienation, with higher scores indicating a more secure parent-child relationship. Peer victimization was measured using the Multidimensional Peer-Victimization Scale (MPVS), where higher scores indicate greater victimization.
At the community and societal level, perceived stress was measured using the Chinese Perceived Stress Scale (CPSS) (6), where higher scores suggest increased perceived stress (
Supplementary Table S1 ). All scales employed in this study demonstrate robust reliability and validity and are extensively utilized within our national context.Descriptive data are presented as medians with interquartile ranges (IQR). The Wilcoxon rank test was employed for univariate analysis to evaluate differences between groups. Multiple linear regression analysis was then conducted to further investigate these factors and assess their collective impact. A network model was developed to estimate the relationships between depressive symptoms and associated factors using the R-package qgraph. In this model, nodes represent depressive symptoms and factors, while edges represent partial correlation coefficients between pairs of nodes. Thicker and more saturated edges indicate stronger correlations. Green edges signify positive partial correlations, and red edges indicate negative correlations. Statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, US) and R Studio software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria). All tests were two-sided and conducted at the 0.05 level of significance.
This study enrolled 1,800 adolescents, out of which 129 were excluded due to missing critical data, such as scores on the CES-DC scale. Consequently, the analysis incorporated 1,671 participants, consisting of 810 boys and 861 girls. The mean age of the adolescents was 14.14±1.62 years. Participants were almost evenly split between educational levels, with 861 (51.53%) attending junior high and 810 (48.47%) attending senior high school. The average CES-DC scale score was 14.88±10.48. Within the population, 444 individuals (26.57%) scored above 20 on the CES-DC scale, indicative of more significant depressive symptoms, whereas 1,227 (73.43%) scored 20 or below.
The results of the univariate analysis revealed significant distinctions in personality dimensions among adolescents with depressive symptoms. Specifically, these adolescents exhibited notably higher scores in neuroticism and psychoticism, and lower scores in extraversion and the lie dimension (P value <0.001). Furthermore, coping styles differed significantly; adolescents with depressive symptoms demonstrated lower scores in positive coping styles and higher scores in negative coping styles (P value <0.001). Environmental factors related to family and school also varied. Adolescents with depressive symptoms reported lower scores in parent-child attachment and higher scores in peer victimization and childhood abuse (P value <0.001). Additionally, at the mezzo level, the perceived stress among these adolescents was significantly elevated (P value <0.001) (Table 1). In the multiple linear regression analysis, which yielded an F-value of 92.32 and accounted for 61% of the variance (R2=0.61, P value <0.001), the retained variables included extraversion, neuroticism, positive coping, negative coping, parent-child attachment, peer victimization, emotional abuse, emotional neglect, and perceived stress (Table 2). Gender-based stratification analyses were also conducted (
Supplementary Table S2 ).Variables Total CES-DC≤20 CES-DC>20 Z P value Age 14 (13–16) 13 (13–16) 15 (13–16) 3.29 0.001 Sex, n (%) 29.76 <0.001 Boy 810 (48.47) 644 (79.51) 166 (20.49) Girl 861 (51.53) 583 (67.71) 278 (32.29) Individual factors Personality Psychoticism 2 (1–4) 2 (1–3) 3 (2–5) 7.37 <0.001 Extraversion 15 (10–17) 15 (11–17) 13 (8–16) −5.62 <0.001 Neuroticism 6 (2–14) 4 (1–9) 15 (8–19) 12.62 <0.001 Lie 16 (12–19) 16 (13–19) 14 (11–17) −7.24 <0.001 Coping style Positive coping 23 (17–28) 24 (20–30) 18 (13–23) −14.05 <0.001 Negative coping 11 (8–15) 10 (8–14) 13 (10–16) 7.59 <0.001 Family and school environment Parent-child attachment 77 (64–90) 81 (68–92) 66 (56–76) −11.67 <0.001 Peer-victimization 4 (0–12) 2 (0–9) 10 (2–26) 8.94 <0.001 Childhood abuse Emotional abuse 6 (5–7) 5 (5–6) 8 (6–11) 17.33 <0.001 Physical abuse 5 (5–5) 5 (5–5) 5 (5–7) 11.53 <0.001 Sexual abuse 5 (5–5) 5 (5–5) 5 (5–5) 6.67 <0.001 Emotional neglect 8 (5–12) 6 (5–9) 12 (8–16) 15.26 <0.001 Physical neglect 6 (5–9) 5 (5–9) 8 (6–10) 11.40 <0.001 Total score 31 (26–39) 29 (26–34) 40 (33–48) 16.77 <0.001 Mezzo level Perceived stress 16 (11–20) 14 (9–18) 20 (16–24) 12.41 <0.001 Abbreviation: IQR=interquartile range; CES-DC=center for epidemiologic studies depression scale for children. Table 1. The score distribution of the influencing factors between depressive symptom groups in Chinese adolescents, median (IQR).
Variables Parameter estimation Standard error t P value VIF Intercept −1.91 3.33 −0.57 0.566 0 Age 0.72 0.19 3.80 <0.001 1.07 Extraversion −0.28 0.07 −3.88 <0.001 1.23 Neuroticism 0.39 0.07 5.98 <0.001 2.22 Positive Coping −0.30 0.05 −6.26 <0.001 1.46 Negative Coping 0.29 0.07 4.13 <0.001 1.39 Peer-Victimization 0.12 0.02 5.82 <0.001 1.19 Emotional Abuse 0.72 0.12 6.16 <0.001 1.48 Emotional Neglect 0.23 0.07 3.13 0.002 1.41 Perceived Stress 0.19 0.06 3.33 0.001 2.29 R2=0.61, F=92.32, P value<0.001 Note: The assumptions required for linear regression were met.
Abbreviation: VIF=variance inflation factor.Table 2. Multiple linear regression analysis for the association between depressive symptoms and multi-dimensional influencing factors among Chinese adolescents.
The network analysis revealed that among the factors influencing depressive symptoms, neuroticism (r=0.24), emotional abuse (r=0.22), and positive coping style (r=−0.23) exhibited the strongest and most direct correlations (P value <0.001). Stress demonstrated a positive correlation with neuroticism and a negative correlation with extraversion. The impact of stress on depressive symptoms appears to be predominantly mediated by personality traits, particularly neuroticism and extraversion, as shown in Figure 1.
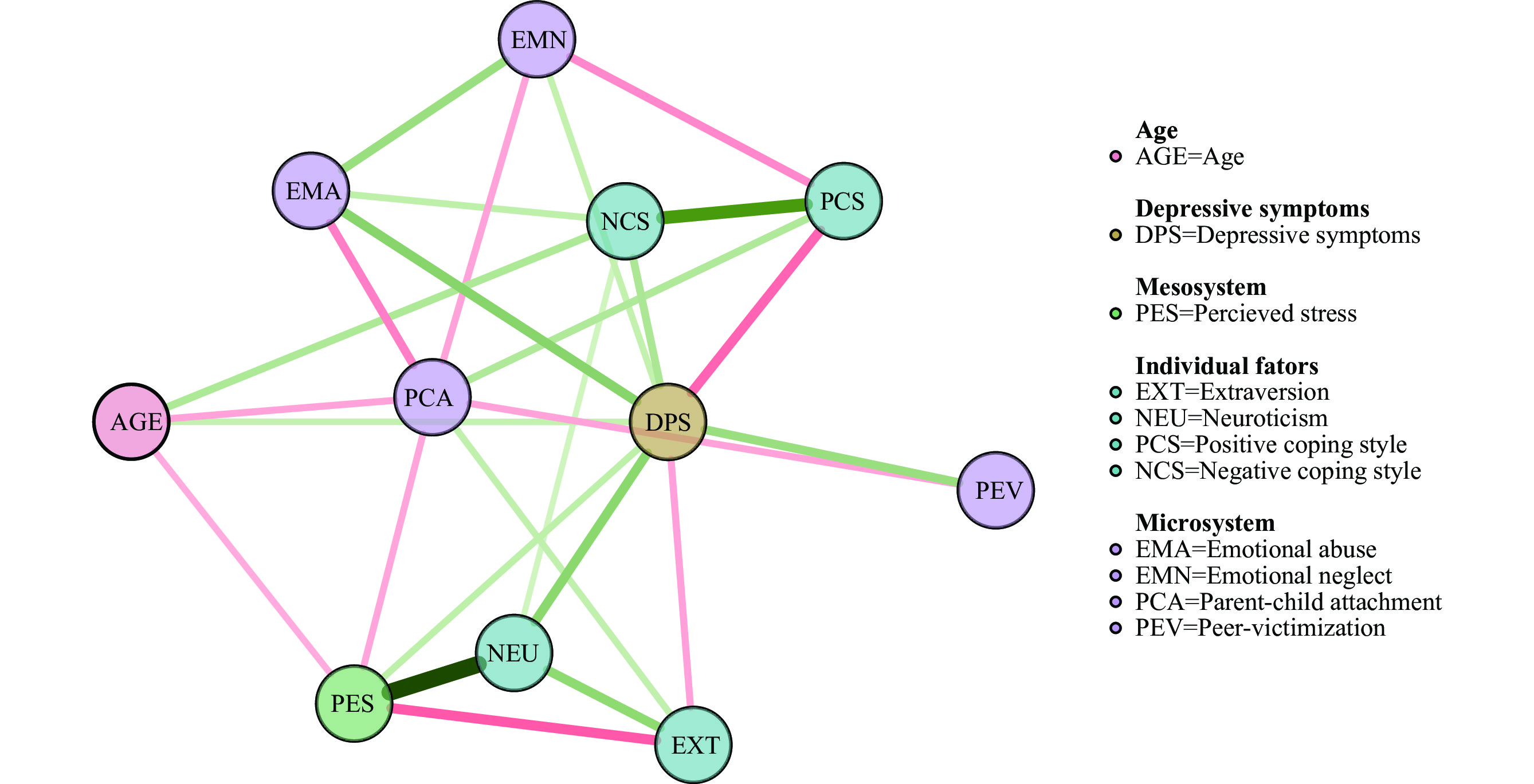 Figure 1.
Figure 1.Network structure of associations between multidimensional influencing factors and depressive symptoms in Chinese adolescents.
Note: Network structures were automatically generated using the “qgraph” package in R. These networks visually represent nodes (which include depressive symptoms and influential factors) and edges (representing pairwise partial correlations among items). In the network, green edges denote positive associations, and red edges denote negative connections. Additionally, the thickness of the lines corresponds to the strength of the associations.
Abbreviation: AGE=age; DPS=depressive symptoms; PES=perceived stress; EXT=extraversion; NEU=neuroticism; PCS= positive coping style; NCS=negative coping style; EMA=emotional abuse; EMN=emotional neglect; PCA=parent-child attachment; PEV=peer-victimization.
-
This study examines the impact of multi-dimensional factors on depressive symptoms in adolescents, guided by ecological systems theory and network structure analysis. Findings suggest that the most direct and potent influences on depressive symptoms occur at the individual level, particularly through traits such as neuroticism and positive coping styles. Furthermore, the relationship between stress and depressive symptoms appears to be primarily moderated by personality traits, notably neuroticism and extraversion.
Our findings indicate that high neuroticism is associated with an increased risk of depressive symptoms in adolescents, while extraversion appears to serve as a protective factor against depression. Furthermore, the network analysis revealed that neuroticism and extraversion inversely modulate the effects of perceived stress. Neuroticism, characterized by heightened negative emotionality and stress reactivity, may enhance stress appraisals and psychological distress, thereby increasing susceptibility to depressive symptoms (7). Conversely, extraversion, which is marked by sociability, assertiveness, and considerable emotional expressiveness, is typically linked with lower stress appraisals and reduced reactivity to stressful events, providing a protective effect against depressive symptoms (8). However, given that personality traits are stable and enduring, altering them to prevent depressive symptoms in adolescents is not a viable approach.
Our research has identified an additional individual factor, the positive coping style, which exerts a significant and direct impact on depressive symptoms among adolescents. A positive coping style entails addressing problems in a direct and rational manner and approaching challenges with an optimistic attitude. This approach can facilitate a sense of accomplishment, thereby promoting psychological health and reducing the prevalence of depressive symptoms. Our findings align with previous research, which has reported that a positive coping style is a protective factor against depression (9). Conversely, a negative coping style, which is characterized by avoidance, withdrawal, and denial, is associated with an increased risk of depressive symptoms. Unlike inherent personality traits, a positive coping style can be developed through education and cognitive behavioral therapy, making it a crucial target for intervention.
Consistent with prior research, our findings confirm that emotional abuse constitutes a particularly detrimental form of childhood maltreatment (10) for the development of depressive symptoms in adolescents. It is hypothesized that exposure to emotional abuse, characterized by statements such as “you are such a stupid child; you are worthless,” can evoke feelings of assault, rejection, and degradation. Accordingly, affected individuals are more likely to develop negative self-perceptions and a pessimistic attributional style, which are known contributors to the onset of depression (11). However, emotional abuse has historically received less attention compared to other types of abuse, such as sexual and physical abuse. This oversight may be attributed to the chronic nature of the damage caused by emotional abuse, which is less immediately apparent and whose impacts are often underestimated. Consequently, there is a pressing need to allocate greater resources and focus toward the prevention of this form of abuse in children and adolescents.
This study is subject to some limitations. First, due to its cross-sectional design, it is impossible to establish causal relationships, and the estimations of network structure should be considered tentative and exploratory. The hypotheses generated by this study require further validation through prospective designs. Second, the sample was recruited exclusively from Beijing, which may limit the generalizability and representativeness of the findings. Future studies with larger, more nationally representative samples are needed to deepen the understanding of these results. Despite these limitations, this study is the first to depict the interrelationships among ecological systems theory-based multi-dimensional factors influencing adolescent depression using network structure. The findings provide valuable insights, offering clearer evidence for the development of more targeted interventions in the future.
In conclusion, a positive coping style has been identified as a critical protective factor against depressive symptoms in adolescents, while neuroticism and emotional abuse were notable risk factors. It is imperative to emphasize parental awareness regarding emotional abuse. Future intervention strategies should prioritize enhancing positive coping mechanisms and mitigating negative ones to bolster adolescents’ mental health resilience.
-
No conflicts of interest.
HTML
| Citation: |

|