

 Download:
Download:




-
Intimate partner violence (IPV) constitutes a significant public health concern with detrimental implications for women’s health (1). Globally, more than one in three women aged 15 years or older has experienced IPV in their lifetime (2). Recent findings indicate that the prevalence of physical and sexual violence among women in China is 40.2% and 11%, respectively (3). While the global burden of IPV has been increasing, China lacks national-level surveillance data on IPV burden. This study assessed the burdens of human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), interpersonal violence, and depressive disorders attributable to IPV among women aged 15 years or older in China, utilizing data from the Global Burden of Disease (GBD) 2019 (4).
In 2019, China reported an estimated 2,398 IPV-attributable deaths, with an age-standardized death rate (ASDR) of 0.3 per 100,000, reflecting an average annual decrease of 3.63% since 1990. IPV-related disability-adjusted life years (DALYs) in China amounted to 789,926, with an age-standardized rate (ASR) of 93.8 DALYs per 100,000, marking an average annual decrease of 1.34% from 1990 to 2019. Age-standardized DALYs rates for HIV/AIDS, interpersonal violence, and depressive disorders attributable to IPV in China were 4.6, 54.1, and 54.5 (per 100,000), respectively. The burden of HIV/AIDS attributable to IPV exhibited a significant upward trend from 1990 to 2019, with annual increases of 4.66% in ASDR and 4.42% in age-standardized DALYs rate. The age groups 30–34 and 50–54 experienced higher IPV burdens compared to other age groups. Public health policymakers must urgently consider the development and implementation of effective interventions for strengthening IPV surveillance and prevention among women in China.
We acquired data on deaths, DALYs, years of life lost (YLLs), and years lived with disability (YLDs) for HIV/AIDS, interpersonal violence, and depressive disorders attributable to IPV among Chinese women aged 15 years or older from the GBD 2019, utilizing the Global Health Data Exchange query tool (
http://ghdx.healthdata.org/gbd-results-tool ). DALYs were computed as the sum of YLLs and YLDs. The GBD 2019 estimates the burden of diseases and injuries in China using data from population registration, national census, mortality registration and reporting systems, disease surveillance systems, systematic review studies, and other sources. The exposure levels of IPV for each age-sex-location-year included in the GBD study were determined based on all available data sources via spatiotemporal Gaussian process regression, DisMod-MR 2.1 (a Bayesian meta-regression method), or alternative methods. Attributable deaths, YLLs, YLDs, and DALYs were computed by multiplying population-attributable fractions (PAFs) by the relevant outcome measure for each age-sex-location-year. Detailed modeling methods can be found in the GBD 2019 supplementary materials (4). In this study, the IPV definition used in GBD 2019 refers to individuals who have experienced one or more acts of physical and/or sexual violence by a current or former intimate partner since the age of 15 years. Age data were extracted in five-year increments for a total of 16 GBD age groups.The ASR per 100,000 individuals was obtained from the GBD database. In the GBD 2019, age standardization was calculated using the Segi world standard population and displayed in 5-year intervals by sex. To assess changing trends over a specified time interval, the estimated average annual percentage change (AAPC) in ASR was calculated, which is commonly used in secondary analyses based on GBD studies (5).
Assuming the natural logarithm of ASR fits a linear regression model
$ {\text{y}} = \alpha + \beta x + \varepsilon $ , y is equal to ln(ASR), and x corresponds to the calendar year. Then, the 95% confidence interval (CI) of the AAPC was determined using the linear regression model. Then,$Estimated\; AAPC=100\times ({e}^{\beta }-1)$ , its 95% CI was estimated using the linear regression model. A statistically significant change was identified if the 95% CI did not intersect zero. The estimated AAPC value represents the annual percentage change. This study utilized the estimated AAPC to investigate the trends of IPV burden by age (15–49, 50–69, and 70+) and diseases/injuries (HIV/AIDS, interpersonal violence, and depression disorders) in China from 1990 to 2019. All data analyses and mapping were conducted using R software (version 3.6.0; R Core Team, Vienna, Austria).From 1990 to 2019, the number of deaths attributed to IPV decreased from 3,921 to 2,398, and the ASDR declined from 0.7 per 100,000 to 0.3 per 100,000, representing an annual average decrease of 3.63% (Table 1). During the same period, the number of DALYs associated with IPV in China increased from 763,110 to 789,926, while the age-standardized DALYs rate decreased from 125.5 per 100,000 to 93.8 per 100,000, showing an average annual decrease of 1.34%. In 2019, age-standardized DALYs rates for HIV/AIDS, interpersonal violence, and depressive disorders related to IPV were 4.6 per 100,000, 54.1 per 100,000, and 54.5 per 100,000, respectively. The ASDRs for HIV/AIDS and interpersonal violence attributable to IPV were 0.1 per 100,000 and 0.2 per 100,000, respectively.
Diseases/injuries Death DALYs Cases (n), 1990 ASR per 100,000, 1990 Cases (n), 2019 ASR per 100,000, 2019 Estimated AAPC 1990−2019 Cases (n), 1990 ASR per 100,000, 1990 Cases (n), 2019 ASR per 100,000, 2019 Estimated AAPC 1990−2019 All 3,921
(2,597 to 5,580)0.7
(0.5 to 1.0)2,398
(1,679 to 3,211)0.3
(0.2 to 0.4)−3.63
(−4.03 to −3.23)763,110
(392,809 to 1,224,332)125.5
(63.5 to 199.5)789,926
(354,381 to 1,304,433)93.8
(44.6 to 153.4)−1.34
(−1.56 to −1.12)HIV/AIDS 70
(8 to 149)0.0
(0.0 to 0.0)751
(376 to 1,270)0.1
(0.1 to 0.2)4.66
(3.68 to 5.65)3,764
(502 to 7,825)0.7
(0.1 to 1.4)32,318
(15,858 to 56,475)4.6
(2.3 to 8.1)4.42
(3.51 to 5.33)Interpersonal violence 3,851
(5,475 to 2,527)0.7
(0.4 to 1.0)1,647
(1,086 to 2,348)0.2
(0.2 to 0.3)−4.59
(−5.01 to −4.16)449,996
(282,928 to 673,978)78.5
(49.3 to 117.5)377,516
(238,421 to 561,538)54.1
(34.2 to 80.5)−1.68
(−1.87 to −1.50)Depressive disorders − − − − − 309,351
(1,241 to 715,826)53.9
(0.2 to 124.8)380,093
(1,480 to 878,531)54.5
(0.2 to 125.9)−1.14
(−1.69 to −0.59)Age group 15–49 years HIV/AIDS 52
(7 to 112)0.0
(0.0 to 0.0)388
(177 to 711)0.1
(0.1 to 0.2)4.88
(3.83 to 5.95)3,170
(444 to 6,749)1.0
(0.1 to 2.1)20,910
(9,451 to 38,470)6.0
(2.7 to 11.0)4.57
(3.58 to 5.57)Interpersonal violence 3,082
(1,917 to 4,507)1.0
(0.6 to 1.4)1,038
(621 to 1,534)0.3
(0.2 to 0.4)−4.74
(−5.28 to −4.20)397,603
(241,127 to 604,037)123.1
(74.6 to 187.0)284,510
(169,717 to 447,950)81.0
(48.3 to 127.6)−1.86
(−2.07 to −1.64)Depressive disorders − − − − − 248,884
(989 to 577,260)77.0
(0.3 to 178.7)190,288
(735 to 431,550)54.2
(0.2 to 122.9)−1.47
(−2.12 to −0.83)50–69 years HIV/AIDS 16
(1 to 34)0.0
(0.0 to 0.0)298
(148 to 490)0.2
(0.1 to 0.3)5.38
(4.34 to 6.42)551
(47 to 1,158)0.7
(0.1 to 1.6)10,123
(4,915 to 16,965)5.5
(2.7 to 9.2)5.51
(4.51 to 6.52)Interpersonal violence 568
(359 to 856)0.8
(0.5 to 1.2)417
(258 to 624)0.2
(0.1 to 0.3)−4.31
(−4.6 to −4.02)43,874
(28,706 to 66,137)59.1
(38.7 to 89.1)75,992
(46,607 to 117,521)41.2
(25.3 to 63.7)−1.43
(−1.58 to −1.29)Depressive disorders − − − − − 51,431
(240 to 129,057)69.3
(0.3 to 173.8)157,568
(725 to 395,024)85.5
(0.4 to 214.2)0.19
(−0.28 to 0.66)70+ years HIV/AIDS 2
(0 to 4)0.0
(0.0 to 0.0)65
(29 to 115)0.1
(0.1 to 0.2)6.59
(5.36 to 7.84)42
(3 to 85)0.2
(0.0 to 0.4)1,285
(562 to 2,292)2.2
(1.0 to 3.9)6.86
(5.86 to 7.87)Interpersonal violence 202
(135 to 297)0.9
(0.6 to 1.4)192
(126 to 288)0.3
(0.2 to 0.5)−3.73
(−4.01 to −3.46)8,519
(5,595 to 12,773)39.2
(25.7 to 58.7)17,013
(10,806 to 26,150)29.0
(18.4 to 44.5)−1.13
(−1.19 to −1.07)Depressive disorders − − − − − 9,036
(35 to 22,893)41.5
(0.2 to 105.3)32,236
(124 to 82,798)54.9
(0.2 to 141.0)0.73
(0.44 to 1.03)Abbreviation: DALYs=disability-adjusted life years; AAPC=average annual percentage change; ASRs=age-standardized rates; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome. Table 1. Deaths and DALYs attributable to intimate partner violence in 1990 and 2019, and estimated AAPC in ASRs per 100,000 in females in China from 1990 to 2019.
From 1990 to 2019, there was a downward trend in deaths, DALYs, YLLs, and YLDs attributable to IPV (Figure 1). However, an opposite trend was observed for HIV/AIDS-related deaths and DALYs attributable to IPV, with the average annual ASR increasing by 4.66% and 4.42%, respectively. Furthermore, a decrease in both deaths and DALYs associated with interpersonal violence due to IPV was found, with the average annual ASR decreasing by 4.59% and 1.68%, respectively. Lastly, the age-standardized DALYs rate for depressive disorders exhibited an annual decrease of 1.14% from 1990 to 2019.
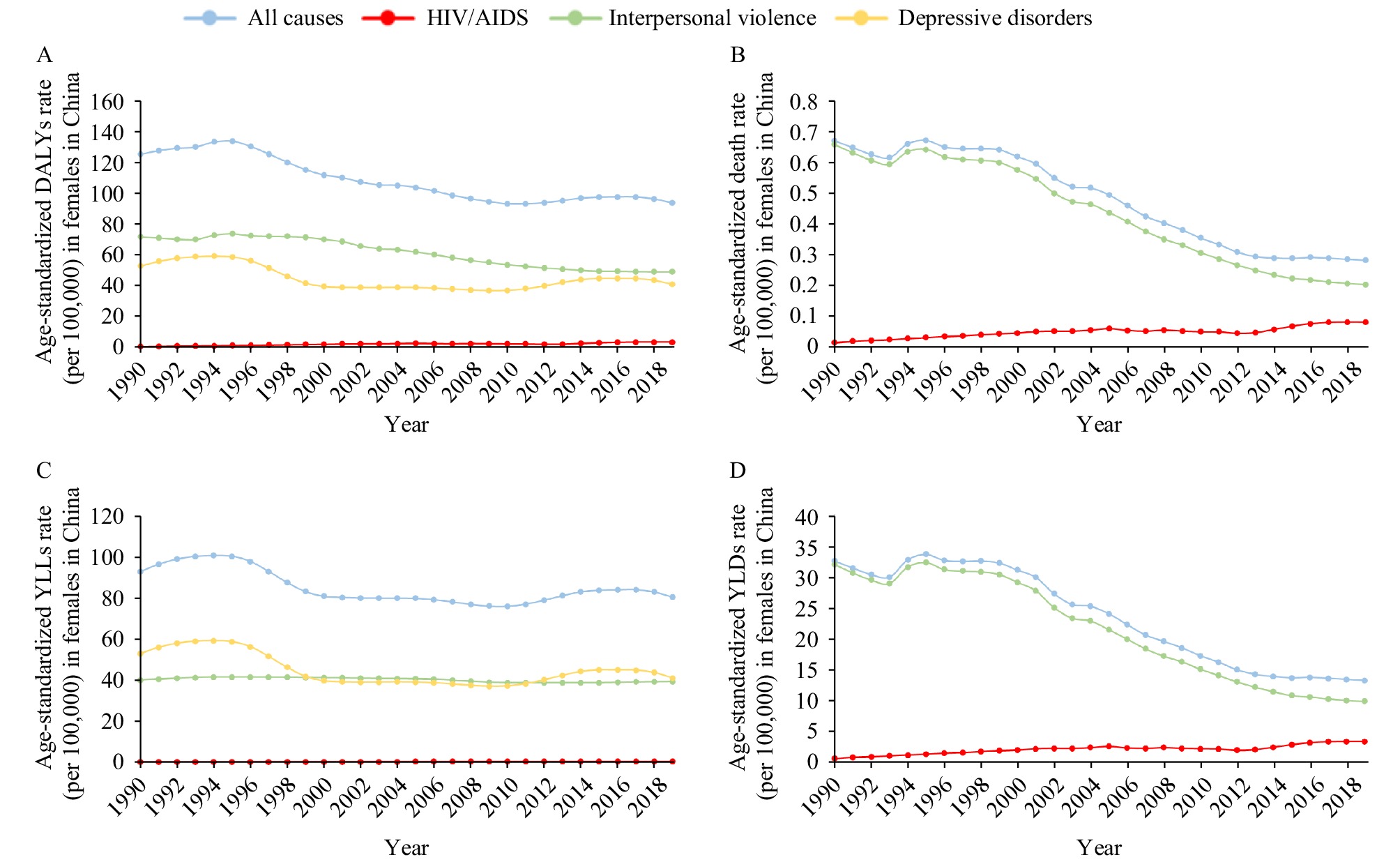 Figure 1.
Figure 1.Trends of diseases/injuries burden attributable to IPV in China, 1990–2019. (A) Trend in the age-standardized DALYs rate. (B) Trend in the ASDR. (C) Trend in age-standardized YLLs rate. (D) Trend in age-standardized YLDs rate.
Abbreviation: IPV=intimate partner violence; DALYs=disability-adjusted by life years; ASDR=age-standardized death rate; YLLs=years of life lost; YLDs=years lived with disability; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome.The highest number of deaths, YLLs, YLDs, and DALYs due to interpersonal violence resulting from IPV appeared in the 30–34 age group; these measures generally decreased as age increased (Figure 2). Among women aged 50–54 years, the highest DALYs and YLDs were caused by depressive disorders attributable to IPV, with a subsequent decline in value as age progressed. For HIV/AIDS related to IPV, the highest DALYs and YLLs occurred in the 30–34 age group. Meanwhile, the highest number of deaths and YLDs linked to HIV/AIDS attributable to IPV were observed in the 50–54 age group and 45–49 age group, respectively. Notably, DALYs resulting from interpersonal violence exceeded those from depressive disorders before the age of 44, with an inverse trend emerging beyond this age.
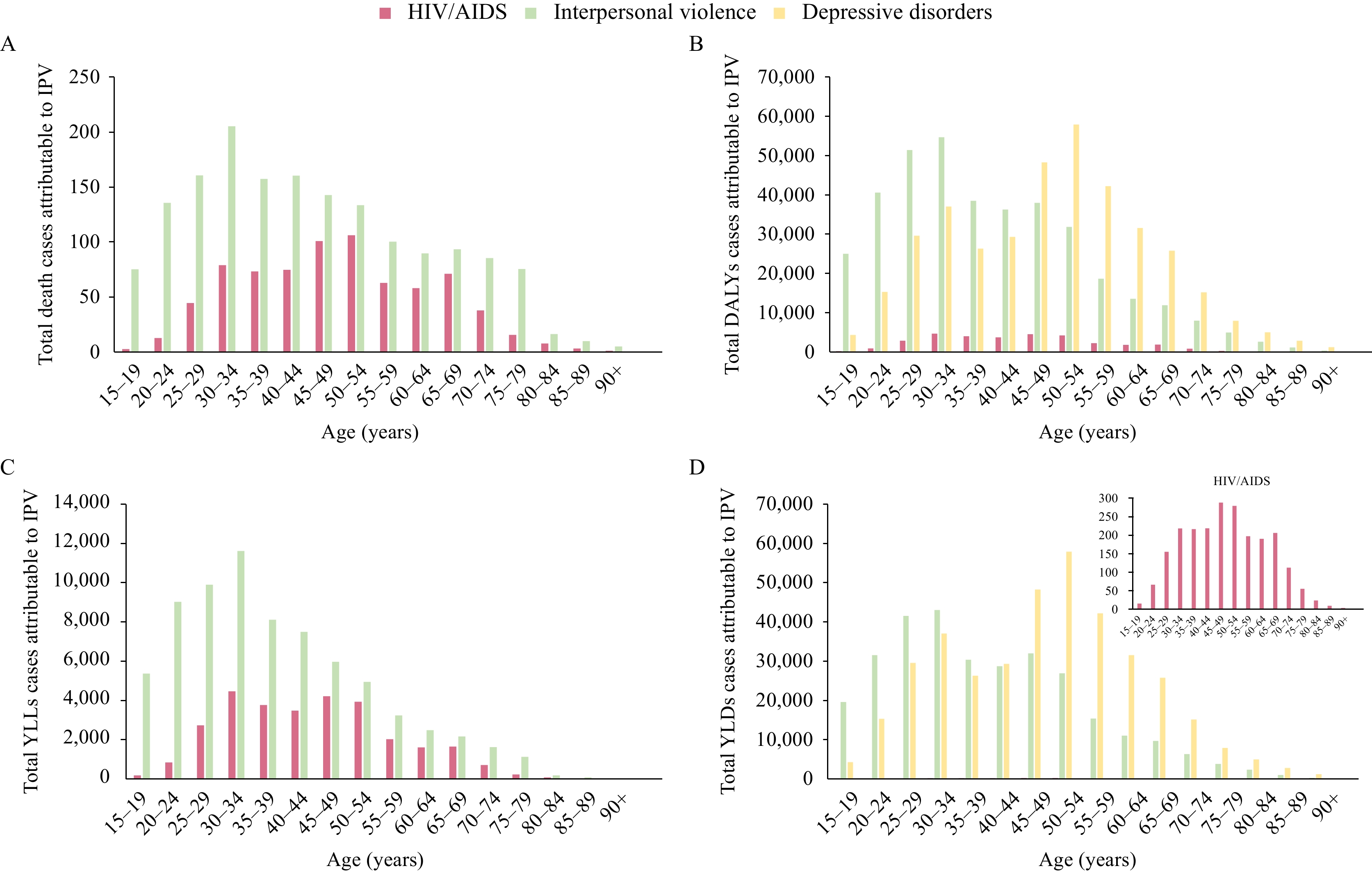 Figure 2.
Figure 2.Overall death, DALYs, YLLs, and YLDs cases attributable to IPV in China by age, 2019. (A) The number of death cases. (B) The number of DALYs cases. (C) The number of YLLs cases. (D) The number of YLDs cases.
Abbreviation: IPV=intimate partner violence; DALYs=disability-adjusted by life years; YLLs=years of life lost; YLDs=years lived with disability; HIV=human immunodeficiency virus; AIDS=acquired immunodeficiency syndrome. -
The present study revealed a decrease in the overall burden of IPV among women aged 15 years or older in China from 1990 to 2019. Nevertheless, an escalating trend was observed in the burden of HIV/AIDS attributable to IPV during the same time frame, with a 4.66% annual increase in ASDR and a 4.42% annual increase in age-standardized DALYs rate. Notably, the age groups of 30–34 and 50–54 experienced a higher IPV burden compared to other age groups.
The observed reduction in IPV prevalence in China may be attributed to advancements in women's rights legislation, educational opportunities, and economic development over the past two decades. Following the adoption of the Beijing Declaration Platform for Action during the United Nations Fourth World Conference on Women in 1995, the Chinese government enacted numerous policies and regulations aimed at eliminating violence against women and promoting gender equality. The Domestic Violence Law of the People’s Republic of China constitutes the nation’s first piece of legislation explicitly prohibiting IPV, extending its application to unmarried cohabiting couples as well (6).
Over time, progress toward gender equality has been made in areas such as employment, education, and entrepreneurial opportunities for women, leading to increased economic independence. This development has been identified as a significant factor in reducing the prevalence of male chauvinism and IPV (7).
Although progress has been made in advancing women’s status in China, rigid gender norms persist, particularly in rural areas (3). Domestic violence, often associated with shame, is regarded as a private issue not to be disclosed to outsiders (8). The current study indicates that the prevalence of IPV in China remains high. Consistent with our findings, Yuan et al. reported a high prevalence of physical violence among women in China (40.2%), significantly higher than that in high-income countries such as Japan (15%) (9). Importantly, the study demonstrates an increasing burden of HIV/AIDS attributable to IPV, a finding in line with research conducted in South Africa (7). This may be attributed to IPV exacerbating HIV prevalence among high-risk women, such as female sex workers (FSWs) and drug users, while also impeding their access to treatment and care. A cross-sectional study in China reported that approximately 58% of FSWs experienced violence from stable partners (10). The findings of this study underscore the need for strengthened HIV intervention efforts among key female populations, emphasizing postexposure prophylaxis, HIV testing, and treatment.
The results of this study revealed that the age groups 30–34 and 50–54 experienced a greater burden of IPV compared to other age groups. As women in China tend to postpone marriage and childbearing, those in the 30–34 age range often encounter fatigue, economic pressures associated with raising a child, and disagreements surrounding child-rearing methods (11). Moreover, women with children are less likely to leave abusive partners. On the other hand, women aged 50 and older may experience emotional instability due to menopause. The age of 50 also coincides with the typical retirement age for Chinese women, and those who are retired tend to report high-severity IPV as a result of increased activity (12).
Our study was subject to several limitations. First, the estimates of the burden attributable to IPV relied on the availability and quality of original data as well as the efficacy of the models used when original data was absent. Second, the study may underestimate the burdens attributable to IPV, as it only evaluated three diseases/injuries associated with IPV and concentrated solely on women aged 15 years or older. Third, the assessment of the IPV burden by province was not possible due to data unavailability. Finally, the IPV burden could not be evaluated by urban/rural regions as such data was neither collected nor estimated in GBD 2019.
The prevalence of IPV in China remains significant, despite a decreasing trend observed over the past few decades. Alarmingly, the burden of HIV/AIDS attributable to IPV is increasing. Unwavering efforts must be made to develop and implement policies and interventions against IPV, safeguard women’s rightful interests, and advocate for gender equality and women’s empowerment in order to eliminate all forms of violence against women.
-
No conflicts of interest.
-
The Institute for Health Metrics and Evaluation (Washington University), the GBD Risk Factors Collaborators and all contributing staff.
HTML


| Citation: |

|