

 Download:
Download:




-
Since the first monkeypox cases were confirmed in England in May 2022 (1), 100 countries worldwide have reported 53,027 confirmed cases and 15 deaths as of September 2 (2). This is the largest and most widespread monkeypox epidemic in the world since monkeypox virus was discovered and identified in 1958, involving the largest number of countries and transmitting primarily in non-endemic countries (3). Moreover, the currently ongoing monkeypox epidemic also has some characteristics that are different from previous outbreaks (4). For example, most cases have a history of sexual contact, with an overwhelming majority of men who have sex with men (MSM) (5). On July 23, the WHO declared the global monkeypox outbreak a Public Health Emergency of International Concern (PHEIC) in order to address the ongoing outbreak with the required urgency (6).
So far, except for three and one imported cases of monkeypox virus infection in Taiwan, China, and Hong Kong Special Administrative Region (SAR), China, respectively (2,7-9), in the mainland of China, the first monkeypox case, who was imported from an European country, was detected and reported in Chongqing on September 14, 2022 (10), indicating that current monkeypox surveillance in the mainland of China was effective. In consideration of the frequent contacts between China and other countries in trade, business, tourism, and overseas study (11-12), the risk of monkeypox being imported into China and subsequently transmitted locally remains. With the rapid development of the monkeypox epidemic in the world, coupled with the gradual recovery of communication between countries, the risk of monkeypox being imported into China may continue to increase.
China has taken a series of proactive measures to respond to the global monkeypox epidemic. In June 2022, the National Health Commission formulated and issued the Monkeypox Diagnosis and Treatment Protocol (2022 Edition) (13) (hereinafter referred to as Protocol) and the Technical Guidelines for the Prevention and Control of Monkeypox (2022 Edition) (14) (hereinafter referred to as Guidelines) to strengthen the detection and reporting of monkeypox patients in medical institutions. The Customs issued its Circular on Preventing Monkeypox from being Introduced into China (Circular No. 65 of the General Administration of Customs in 2022) (15), further tightening controls over the quarantine of people and animals entering China and surveillance of animal reservoirs.
To achieve the goal of early detection of cases and timely blocking of possible transmission, based on the epidemic situation of monkeypox abroad and the risk of importation into China, China's current surveillance strategy focuses on early detection of imported cases and subsequent transmission, increasing the sensitivity of surveillance, and syndromic surveillance of target populations (Figure 1).
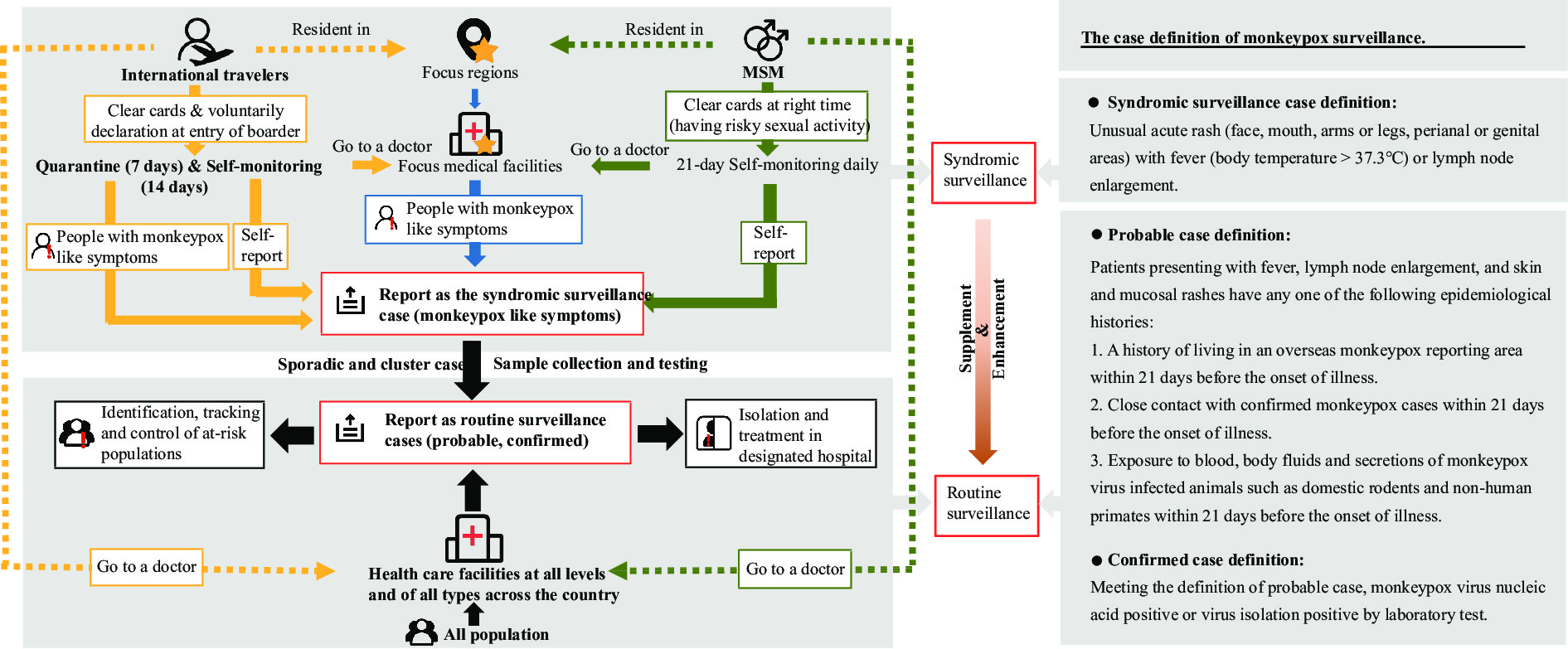 Figure 1.
Figure 1.The framework and the case definition of monkeypox surveillance in the mainland of China, 2022.
Abbreviation: MSM=men who have sex with men. -
As monkeypox virus infection has already been imported and detected in the mainland of China (10) and the COVID-19 prevention and control is still under great pressure, surveillance of symptoms of monkeypox cases in focus populations, medical facilities and regions is an important supplement to the routine surveillance of probable and confirmed monkeypox cases, which is carried out in health care facilities at all levels and of all types across the country (Table 1).
Surveillance scope and coverage Objects or locations of surveillance Contents of surveillance Focus populations International travelers and MSM 1) People coming from abroad are asked to voluntarily declare to the customs at the entry of border
2) People coming from abroad are quarantined at a designated hotel for 7 days after entry
3) People coming from abroad are asked to do a self-monitoring for 14 days after completing the 7-day quarantine at hotel
4) MSM are asked to do a 21-day self-monitoring daily after having any risky sexual activityFocus medical
facilitiesDermatology hospitals, dermatology clinics and STD clinics, including VCT clinics Doctors and nurses monitor whether patients visiting facilities develop monkeypox-like symptoms, and then promptly report to jurisdictional CDC Focus regions Provincial capitals (including municipalities directly under the Central Government) Implement syndromic surveillance in focus medical facilities in provincial capitals or municipalities Across the country Healthcare facilities at all levels and of all types 1) Doctors and nurses monitor whether patients visiting facilities at all levels and of all types meet diagnosis definition of probable and confirmed monkeypox cases, and then promptly report to jurisdictional CDC
2) Both sporadic and cluster cases meeting the definition of monkeypox syndromic surveillance are promptly reportedAbbreviation: MSM=men who have sex with mem; STD=sexually transmitted disease; VCT=HIV voluntary counseling & testing; CDC=center for disease control and prevention. Table 1. Monkeypox surveillance scope, target, object, location and content in the mainland of China, 2022.
-
The focus populations include international travelers and MSM. First, international travelers are asked to voluntarily declare to the customs at the border entry whether they have any monkeypox-like symptoms or any epidemiological exposure history, such as close contact with someone infected with monkeypox. Second, international travelers are required to have a 7-day quarantine at a designated hotel, in which they will be monitored for monkeypox-like symptoms. Third, international travelers are asked to do self-monitoring for monkeypox-like symptoms for 14 days after they have completed the 7-day quarantine at hotel and to promptly report any possible symptoms to the local CDC.
In addition, given the high proportion of cases involving MSM in the current monkeypox epidemic (16) and the clear role of sexual contact and having multiple sexual partners in the spread of monkeypox (17-18), although no domestic transmission has been detected in the mainland of China at present, from a forward-looking perspective of monkeypox surveillance, in addition to the international travelers, MSM are also included in focus populations in focus regions to improve the sensitivity of surveillance for case detection. MSM are asked to do daily self-monitoring for 21 days after having any risky sexual activity and promptly report possible infection to the local CDC.
-
Focus medical facilities mainly include dermatology hospitals, dermatology clinics, and sexually transmitted disease (STD) clinics, including HIV Voluntary Counseling & Testing (VCT) clinics. As in the monkeypox case series, most persons presented with a rash, and the most common anatomical sites were the anogenital area, the trunk, arms, legs, and the palms or soles (19), these medical facilities are considered the focus for monkeypox surveillance to improve the probability of detection.
-
Considering the distribution of ports of entry, mobility of people, MSM population size and activity, and China’s efforts in relevant disease prevention and control, all provincial capitals (including municipalities directly under the Central Government) are selected as areas for monkeypox syndromic surveillance in medical facilities.
-
Three types of case definition are used (Figure 1). Probable cases and confirmed cases are defined clearly in the Protocol (13), but the clinical manifestations defined in the Protocol are too technical and are more applicable to clinical diagnosis instead of surveillance; furthermore, the epidemiological history in the definition is too concerned with overseas exposures. Therefore, on the basis of the definition in the Protocol, the simplified and more sensitive description of monkeypox-like symptoms is adopted for syndromic surveillance case definition in the country: unusual acute rash (face, mouth, arms or legs, perianal or genital areas) with fever (body temperature >37.3 ℃) or lymph node enlargement.
-
Given the potentially large populations of international travelers and MSM, and unknown prevalence of monkeypox virus, clear cards are issued to international travelers at the border entry and to MSM at right time, letting them carry out a self-monitoring for a period of 21 days after entering the country or having a risky sexual activity, respectively, consistent with the maximum incubation period of monkeypox virus infection (20).
The process of self-monitoring is equivalent to the publicity and education of monkeypox prevention and control knowledge. In the focus regions, media campaigns and other means are used to increase MSM education on symptoms of monkeypox, so that they can carry out self-monitoring of monkeypox-like symptoms, and avoid unprotected sex to prevent the risk of monkeypox virus infection and transmission.
-
Although no domestic monkeypox case has yet been reported, the risk of importation has still been the major challenge of monkeypox in the mainland of China. Provincial capitals or municipalities were selected to carry out monkeypox syndromic surveillance as they have more immigrants, more active MSM personnel, and strong diagnostic, treatment, and detection capabilities in hospitals and clinics. Syndromic surveillance is implemented at dermatology hospitals, dermatology clinics, or STD clinics, including VCT clinics in provincial capitals or municipalities.
-
Monkeypox syndromic surveillance is a supplement and enhancement to routine surveillance. According to the Protocol, doctors and nurses monitor whether patients visiting facilities at all levels and of all types meet diagnostic criteria of probable and confirmed monkeypox case, and then promptly report these cases to jurisdictional CDC. In addition, both sporadic and cluster cases meeting the definition of monkeypox syndromic surveillance are also promptly reported across the country. Secondary monkeypox cases will follow the same procedures as the primary cases, and be given a thorough field epidemiological investigation.
-
Monkeypox virus is a Biosafety Level 1 pathogen in China (21), for patients with monkeypox-like symptoms and probable cases, inactivated throat swabs are first collected for biosafety and efficiency. If throat swabs of individuals who have monkeypox-like symptoms are negative, specimens of the skin rash will be sampled for diagnosis. If the laboratory test is positive, multiple non-inactivated specimens, including specimens of skin rash, herpes surface or exudate, blister fluid, scab or scleroderma, will be collected immediately for subsequent work such as virus isolation and gene sequencing. Serum samples during the acute phase (within 7 days of onset) and the convalescent phase (2–3 weeks apart) respectively will be collected for antibody testing.
It is necessary for medical facilities and CDCs at all levels in the mainland of China to establish a stable and sustainable capacity of nucleic acid testing for detection of monkeypox virus as soon as possible. The National Institute for Viral Diseases Control and Prevention (IVDC) of China CDC has developed a nucleic acid testing method for detection of monkeypox virus, completed the development of nucleic acid detection reagents, and distributed the first batch of monkeypox virus detection reagents to provincial CDCs in the mainland of China in August, 2022. At present, many domestic reagent companies have initiated research, development, and production of test kits for monkeypox virus.
-
According to the Protocol (13) and the Guidelines (14), probable cases should be transferred to designated medical facilities for cubicle treatment, and the identification, tracking, and control of at-risk populations should be carried out immediately. Groups of experts on monkeypox diagnosis should be established at all levels of medical facilities and health authorities to study probable cases so as to improve the specificity of monkeypox surveillance and the accuracy of monkeypox diagnosis and to avoid excessive response or waste of epidemic control resources. The medical facilities first organize resident expert group consultations when they detect monkeypox-like symptoms or probable cases, and then, if necessary, refer to local or superior expert groups for consultations.
-
China’s current monkeypox surveillance strategy and implementation plan are based on the current global monkeypox epidemic and domestic situation and subject to timely adjustment according to changes in the characteristics of monkeypox virus and disease, the situational changes of surveillance implementation, case reports in China, and strategic changes to prevent and control infectious diseases.
HTML
Focus Populations
Focus Medical Facilities
Focus Regions
At-Risk Populations: Self-Monitoring and Active Reporting
Focus Regions and Focus Medical Facilities: Combination
Across the Country: Routine and Syndromic Surveillance, Targeting Both Sporadic and Cluster Cases
Specimen Collection and Testing
Considerations for Diagnostic and Reporting Processes
FootNote
| ① | No conflicts of interest. |
| Citation: |

|