

 Download:
Download:




-
Adverse childhood experiences (ACEs) refer to stressful or traumatic events that children may suffer before age 18 and are highly prevalent worldwide. Studies on ACEs indicate that stressful childhood experiences (e.g., child maltreatment, household challenges, peer victimization, and community challenges) are linked to poor health outcomes and health behaviors in adulthood (1). Mental health outcomes, particularly depression, may occur more often in the population with ACEs. Importantly, ACEs have repeatedly been found to increase the risk of mental health problems following development (2). In China, the prevalence of depression has aggressively increased to 20% among the elderly population (3). However, few studies have investigated the association between ACEs and depression in adulthood in China. Therefore, this study aimed to examine the association between ACEs and depressive symptoms and the development trajectories among the middle-aged and elderly in China. We used data from the Chinese Health and Retirement Longitudinal Study (CHARLS). Overall, individuals’ trajectories of depressive symptoms showed an increasing trend. ACEs and their specific domains were associated with each individual’s depressive symptoms. This study emphasizes the long-term relationship between ACEs and depressive symptoms among middle-aged and elderly and encourages policies to promote better early ACEs prevention and intervention.
The CHARLS was conducted by the National School of Development at Peking University, a nationally representative, multi-disciplinary, and public dataset focused on Chinese families and individuals aged 45 and above. The CHARLS utilized a multi-stage stratified probability-proportional-to-size sampling (PPS) technique to select participants. The detailed design of the CHARLS has been reported previously (4). The institutional review board of Peking University has approved the CHARLS study, and all participants of CHARLS have signed consent forms before the face-to-face interview. The four waves of CHARLS in 2011 (Baseline), 2013, 2015, and 2018, along with 2014 life-history data, were used in this study. Finally, 9,069 individuals who had completed all the five surveys (reported no losses to follow-up and missing values) were included in this study.
Depressive symptoms were measured using the Center for Epidemiological Studies Depression Scale-10 (CESD-10) in the CHARLS questionnaire. The CESD score (range 0–30) is a summation of responses to 10 statements, for which participants rate their feelings and behaviors one week before the interview date. Higher CESD scores indicate greater depressive symptoms.
ACEs exposures were retrospectively collected by the 2014 life-history questionnaire. This study defined ACEs according to the original ACE questionnaire and additional recommended items from other studies (5). A total of 18 ACEs items on 4 specific domains were collected, including child maltreatment (emotional neglect, physical abuse, domestic violence, and domestic verbal violence), household challenges (household substance abuse, household mental illness, parental separation or divorce, parental incarceration, household financial adversity, household food deprivation, family member physical health problems, parental death, sibling death), peer victimization (physical bullying and peer rejection), community challenges (community safety, and community hygiene). All the items were dichotomized and summed, thus creating an ACEs score ranging from 0 to 18 (higher scores indicating greater adversity level) and four specific ACEs domains scores.
The individual’s trajectory in adulthood depressive symptoms was investigated by fitting a growth curve model with two levels. Furthermore, this study examined the association between ACEs and depression symptoms. Finally, adjusted coefficients and trajectories were estimated after adjusting for the potential confounding variables, including age, sex, marital status, region, education level, smoking, alcohol drinking, social participation, and self-report of health. All the statistical analysis was carried out by R (version 4.1.0, R Development Core Team, Vienna, Austria).
Supplementary Table S1 shows baseline characteristics of participants. Figure 1 presents the trajectories of depressive symptoms from 2011 to 2018, and Figure 2 presents the trajectories of depressive symptoms by different ACEs domains.Supplementary Table S2 further demonstrates depressive Symptom Scores of the participants by different ACEs domains. Overall, the depressive symptoms were increasing from 2011 to 2018 and the changing patterns over time were similar at different ACEs score levels. The patterns of CESD-s score variation at the different levels indicated that higher ACEs exposure groups displayed higher depressive symptoms than lower ACEs exposure groups. Besides, exposure to higher specific ACEs domains, namely, child maltreatment, household challenges, peer victimization, and community challenges, was associated with a more significant gradient in depressive symptoms trajectories.Supplementary Table S3 further demonstrates the interaction between ACEs and survey year on depressive symptoms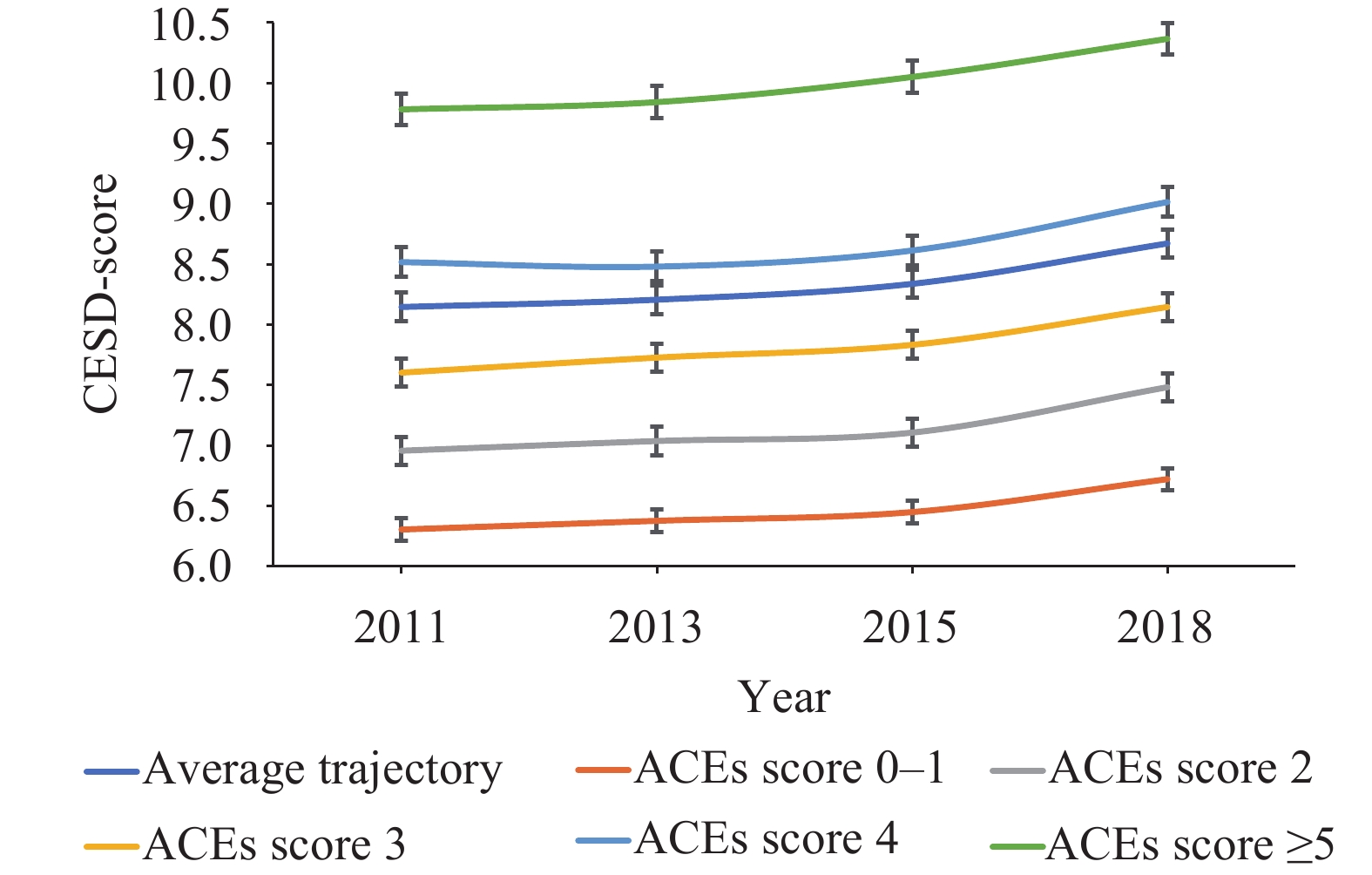 Figure 1.
Figure 1.Predicted trajectories of depressive symptoms by ACEs score, China, 2011–2018.
Note: Results are based on model 1 in Table 1. ACEs score 0–1, ACEs score 2, ACEs score 3, ACEs score 4, and ACEs score ≥5 stand for different ACEs levels (higher scores indicating greater adversity level). ACEs score 4 and ACEs score 5 and above displayed higher depressive symptoms trajectories than average trajectory.
Abbreviations: ACEs=adverse childhood experiences; CESD=Center for Epidemiological Studies Depression.
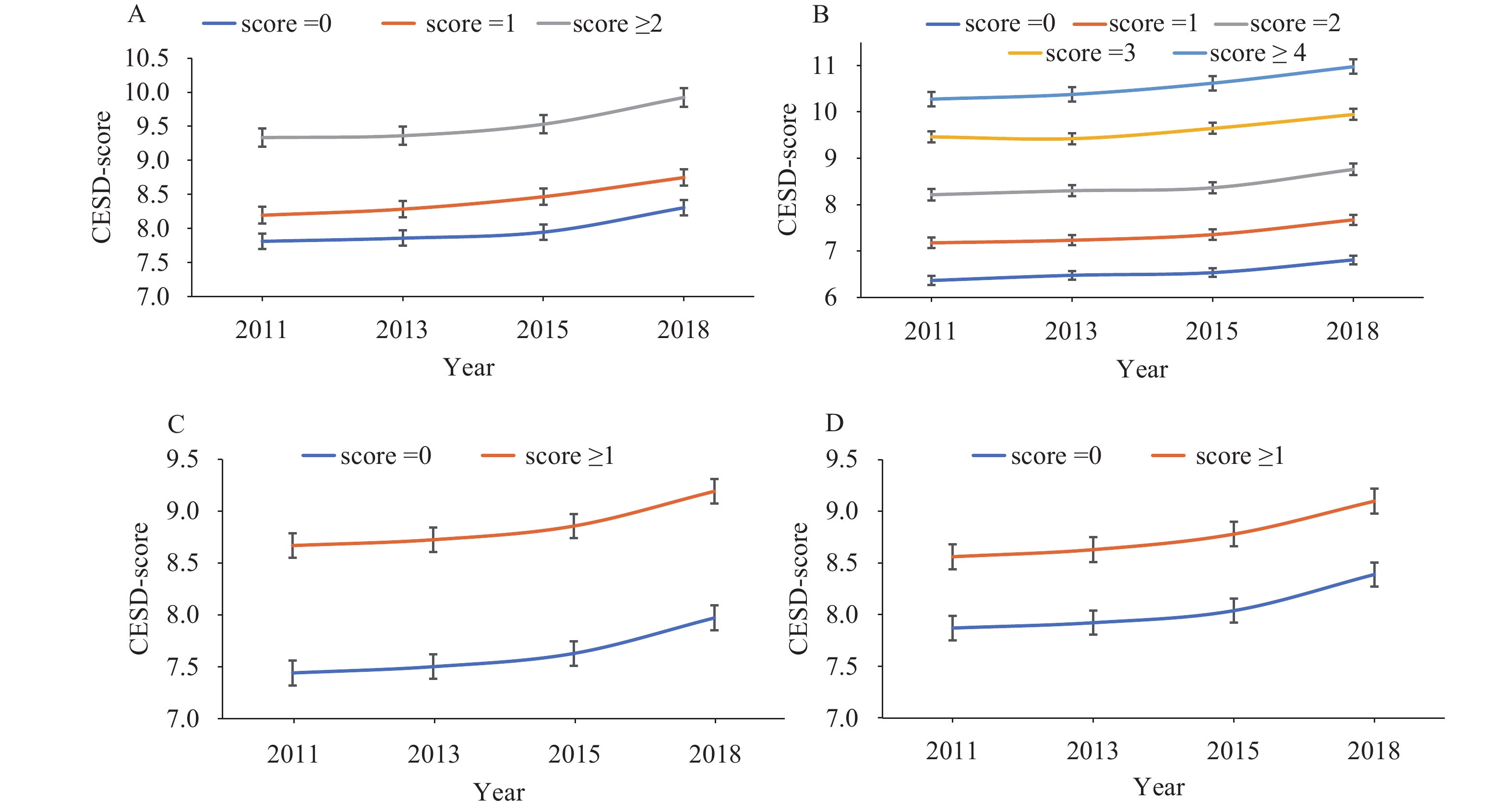 Figure 2.
Figure 2.Predicted trajectories of depressive symptoms by different ACEs domains, China, 2011–2018. (A) Child maltreatment; (B) Household challenges; (C) Peer victimization; (D) Community challenges.
Note: Results are based on model 2 to 5 in Table 1, respectively. Four specific ACEs domains scores were collected based on a total of 18 ACEs items on 4 specific domains. All the items were dichotomized and summed, thus creating a score (higher scores indicating greater adversity level).
Abbreviations: ACEs=adverse childhood experiences; CESD=Center for Epidemiological Studies Depression.
Table 1 presents the results of the association between ACEs and adulthood depressive symptoms. The results showed a significant and consistent increase in depression symptoms scores with cumulative ACEs exposure. Individuals with ACEs scores 2, 3, 4, and ≥5 had 0.27, 0.85, 1.50, and 2.50 point higher depressive symptoms scores than those with 0–1 ACEs scores, respectively. Regarding specific ACEs domains, exposure to higher child maltreatment, household challenges, peer victimization, and community challenges was associated with higher depressive symptoms scores.
Variables Beta 95% CI P-value Model 1 ACEs score 0–1 Ref. 2 0.27 (−0.02 to 0.57) 0.072 3 0.85 (0.56 to 1.10) <0.001 4 1.50 (1.20 to 1.80) <0.001 ≥5 2.50 (2.20 to 2.80) <0.001 Model 2 Child maltreatment score 0 Ref. 1 0.35 (0.17 to 0.54) <0.001 ≥2 1.30 (1.10 to 1.60) <0.001 Model 3 Household challenges score 0 Ref. 1 0.56 (0.29 to 0.84) <0.001 2 1.29 (1.00 to 1.60) <0.001 3 2.22 (1.90 to 2.50) <0.001 ≥4 2.79 (2.40 to 3.10) <0.001 Model 4 Peer victimization score 0 Ref. ≥1 0.74 (0.56 to 0.91) <0.001 Model 5 Community challenges score 0 Ref. ≥1 0.60 (0.43 to 0.77) <0.001 Note: Separate models were estimated for the ACEs and its four specific domains. All the models were adjusted for age, sex, marital status, region, education level, smoking, alcohol drinking, social participant, and selfs-report of health.
ACEs and four specific ACEs domains scores were collected based on a total of 18 ACEs items on 4 specific domains. All the items were dichotomized and summed, thus creating a score (higher scores indicating greater adversity level).
Abbreviations: ACEs=adverse childhood experiences; CI=confidence interval.Table 1. Association between ACEs and depressive symptoms among middle-aged and elderly, China, 2011–2018.
-
This study used a longitudinal design and estimated the trajectories of depressive symptoms at the population level from 2011 to 2018 among the middle-aged and elderly in China. The results showed an increasing trend of depressive symptoms trajectory, and ACEs exposures were associated with the risk of depressive symptoms in the middle-aged and elderly. This study contributes to the present knowledge about the temporal trajectories of depressive symptoms and how these associations varied between ACEs and their specific domains.
A prior study found enduring effects of ACEs on mental health in adulthood (6). People who were verbally abused in childhood have a 1.6 times higher risk of depressive symptoms (7); those with a family history of mental illness had the highest risk of depression (8). These findings on specific domains of ACEs (i.e., child maltreatment and household challenges) were consistent with our study. There are several possible underlying mechanisms behind our findings. Firstly, psychologically, exposure to ACEs could increase negative self-cognition, the likelihood of a behavioral response that exacerbates a threat in the environment, and negative beliefs about self-worth, affecting coping strategies for stressful life events. Secondly, biologically, exposure to ACEs (and even prenatal stress exposure) may permanently alter biological systems, including brain functioning, endocrine, and immune systems, and these changes can exert long-term effects on later mental health. Finally, behaviorally, ACEs could increase the risk of developing unhealthy behaviors, including drug and alcohol use, negative eating patterns, and avoidance of stressful experiences, people, and situations. Also, ACEs are associated with decreased adaptive coping skills (i.e., active coping, emotional support, planning, and reframing). These psychosocial, behavioral, and biological factors then work independently and interactively to increase the risk of depressive symptoms (9).
This study had several strengths. First, this study utilized large national representative datasets from 2011 to 2018, providing a valid and reliable result. Second, a growth curve model was used to estimate the trajectories of depressive symptoms from 2011 to 2018, which could help us understand the trend of depression in the Chinese population. Third, the association between ACEs and depressive symptoms in adulthood was investigated, providing more evidence on this research area and future public health policymaking.
Limitations also need to be acknowledged. First, ACEs were assessed retrospectively, in which potential recall bias existed. However, unlike some subjective measurements, ACEs are less likely to be forgotten. Besides, research has reviewed the evidence of the validity of retrospective reports of ACEs and concluded that such bias is not sufficient to invalidate retrospective data (10). Second, due to the nature of the observational study, we cannot ascertain the causal relationship between ACEs and depressive symptoms.
Therefore, future public health efforts to promote mental health might include reducing the prevalence of ACEs in the population and supporting those who have experienced adverse sequelae as a function of ACEs. Moreover, building a surveillance system on ACEs in China is essential to collect, analyze ACEs data, and support the implementation of ACEs primary prevention strategies.
-
The China Health and Retirement Longitudinal Study (CHARLS) team.
-
No conflicts of interest.
HTML
| Citation: |

|