

 Download:
Download:




-
Efficient surveillance information systems are essential for the prevention and control of infectious diseases. Wulanchabu City Center for Endemic Disease Prevention and Control (WCEDC) established the Brucellosis Integrated Information System (BIIS) in 2013 to make case diagnosis, treatment, and management more effective and reduce the workload of clinicians for inputting data. This was the first time an integrated information system management for brucellosis diagnosis, treatment, and follow-up was developed and implemented. However, the system had not been systematically evaluated and promoted so far. The aim of this study was to evaluate the BIIS using the framework and index of surveillance information system evaluation issued by World Health Organization (WHO). The results indicated that the implementation of the BIIS had significantly improved the efficiency of brucellosis reporting and follow-up management. However, the stability and completeness of the BIIS needs to be further improved. The study demonstrated the pros and cons of this BIIS that could provide evidence for further improvements.
Brucellosis is an infectious-allergic zoonosis caused by Brucella bacteria (1). Brucellosis incidence has been increasing over the past decade with a peak in 2014, especially in the northern China, such as Inner Mongolia, Shanxi, Xinjiang, etc. (2). The surveillance system of brucellosis now primarily consists of National Notifiable Disease Report System (NNDRS) and active surveillance based on the National Brucellosis Surveillance Work Program (NBSWP) in 19 key endemic areas (3-4). The data collecting primarily relied on manual input by medical staff in hospitals or local CDCs, and an effective information network with the Hospital Information System (HIS) or Laboratory Information System (LIS) had not been established. WCEDC was the main medical institute, responsible for local brucellosis case diagnosis and treatment with about 5,000 cases reported per year in Wulanchabu City, Inner Mongolia. The BIIS has been developed and put into use in WCEDC since 2013, which integrated the data of every patient in the HIS and LIS and made the case follow-up management more efficient (Figure 1). The WHO proposed that the surveillance information system needed to be evaluated comprehensively on a regular basis (5). Therefore, this study aimed to evaluate the BIIS by using the framework and index of surveillance information system evaluation released by WHO to detect the pros and cons of the system and provide evidence for further improvement.
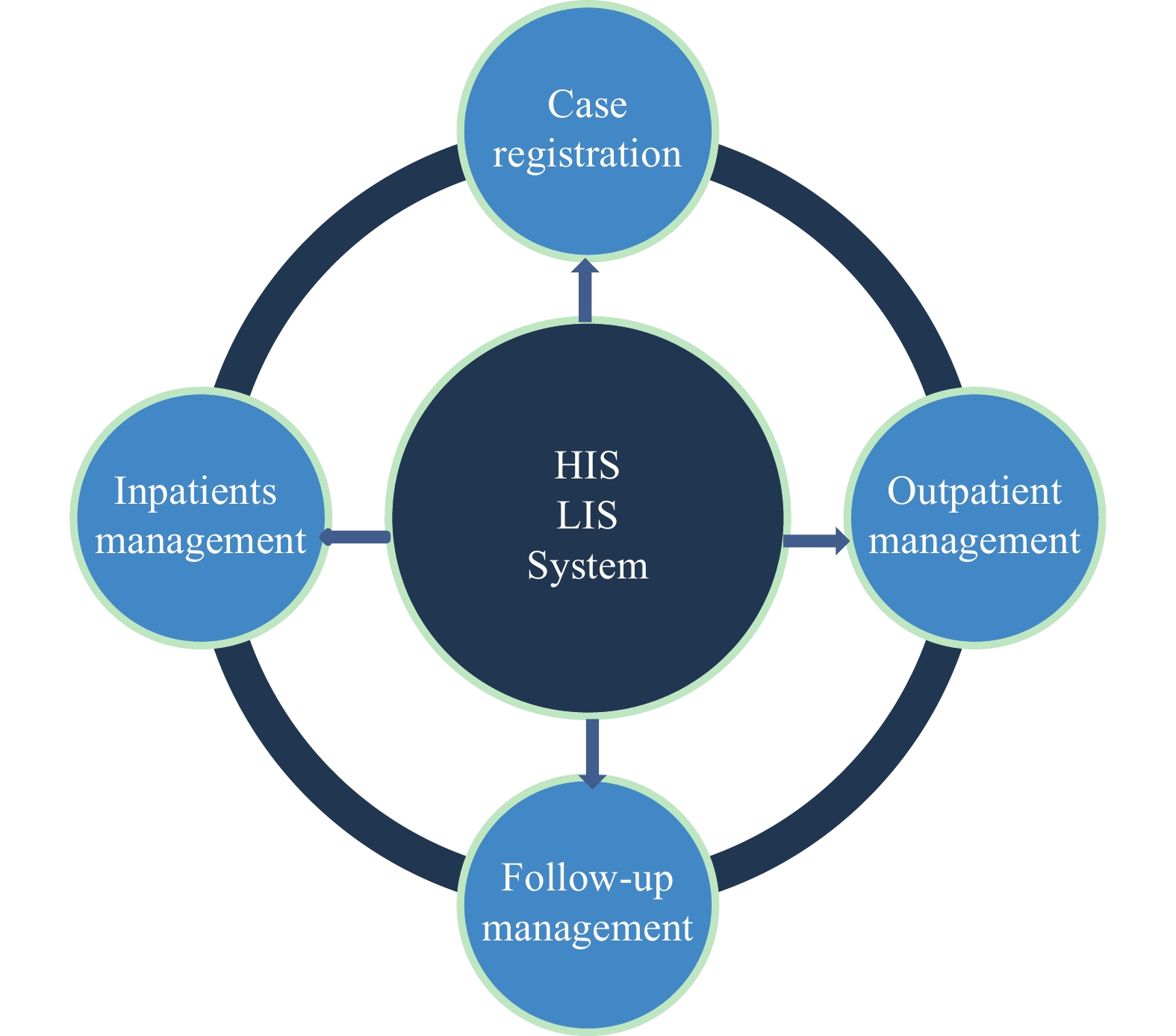 Figure 1.
Figure 1.Function chart of Brucellosis Integrated Information System in Wulanchabu City Center for Endemic Disease Prevention and Control in 2019.Abbreviations: HIS=Hospital information system; LIS=Laboratory information system.
The project was carried out in WCEDC and the data was collected and reported to the BIIS and the NNDRS from March 18 to December 18, 2019. The promptness of reporting was analyzed by comparing the time interval between case diagnosis and reporting in 2019 and that in 2016–2018, and promptness was defined as the interval being less than 24 hours. It was also assessed by comparing cases reported from WCEDC using BIIS with the other nearby institutes, including Tongliao City Center for Endemic Disease Prevention and Control (TCEDC) and Wulanchabu Central Hospital (WCH), both reporting cases without BIIS during the same period. Completeness and accuracy were tested by 12 indicators in the case records. Usefulness was defined as BIIS assisting with the diagnosis, treatment, and management of brucellosis. To evaluate the usefulness of BIIS, it was necessary to evaluate the function of BIIS to determine whether it could meet the actual needs of brucellosis management. The attribute indexes involving simplicity, stability, and acceptability was assessed through a questionnaire, and all the medical staff who operated the BIIS in WCEDC were interviewed at the end of the evaluation project.
The original data from the BIIS and NNDRS was sorted using Microsoft Excel software (version 2010, Microsoft Office, CA, USA) and analyzed usingIBM SPSS Statistics 22.0 (IBM Corp; Armonk NY, USA). Wilcoxon Rank Sum Test was used to compare the medians of the interval between diagnosis and reporting, and chi-squared test was used to compare the promptness proportion. P-value less than 0.05 was considered as statistically significant.
A total of 342 cases were reported in 2019 with a promptness rate of 100% in WCEDC, whereas 210 cases were reported during the same period in 2016–2018 with a promptness rate of 99.05%. The maximum, median, and minimum values of the interval between case diagnosis and reporting in 2019 were 83.36%, 50.00%, and 63.29% less than that in 2016–2018, respectively (Table 1). The comparison analysis of the promptness rate of brucellosis reported in WCEDC, TCEDC, and WCH showed that the median of interval in WCEDC (1.15 h) was significantly lower than that in WCH (17.12 h) and TCEDC (5.17 h). The proportion of cases reported within 2 hours by WCEDC was 69.30%, whereas that by WCH and TCEDC were 33.33% and 1.88%, respectively. The implementation of BIIS had significantly improved the efficiency of brucellosis reporting (Table 2).
Time interval from diagnosis to reporting 2019 (N=342) Average of 2016–2018 (N=210) Change (%) Median (h) 1.15 2.30 −50.00 IQR (h) 4.39 0.85 416.47 Minimum (h) 0.29 0.79 −63.29 Maximum (h) 7.42 44.59 −83.36 <2 h 237 (69.30%*) 108 (51.43%) 34.75† 2–24 h 105 (30.70%) 100 (47.62%) −35.53† ≥24 h 0 (0%) 2 (0.95%) −100.00† Abbreviation: IQR=Inter quartile rang.
* The value in the bracket means the correspondent proportion.
† The percentage of changes for the correspondent proportion.Table 1. Promptness of brucellosis reporting during 2019 and during 2016–2018 in Wulanchabu City Center for Endemic Disease Prevention and Control.
Time interval from diagnosis to reporting WCEDC (N=342) WCH (N=333) TCEDC (N=1,062) P Median (h) 1.15 17.12 5.17 <0.01† IQR (h) 4.39 16.88 0.62 Minimum (h) 0.29 0.20 1.15 Maximum (h) 7.42 22.23 29.27 <2 h 237 (69.30%*) 111 (33.33%) 20 (1.88%) <0.01 2–24 h 105 (30.70%) 222 (66.67%) 1,041 (98.03%) <0.01 ≥24 h 0 (0%) 0 (0%) 1 (0.09%) Abbreviations: WCEDC=Wulanchabu City Center for Endemic Disease Prevention and Control; TCEDC=Tongliao City Center for Endemic Disease Prevention and Control; WCH=Wulanchabu Central Hospital.
* The value in the bracket means the correspondent proportion.
† The difference statistically significant.Table 2. Promptness of brucellosis reporting during the projects of WCEDC, WCH, and TCEDC in 2019.
The results showed that the completeness rate of NNDRS in BIIS was 100% (1,345/1,345), and the accuracy rate was 98.36% (1,323/1,345). However, the completeness rate of the NBSWP in the BIIS was only 33.90% (456/1,345) and accuracy rate was 99.56% (454/456).
Overall, 90.91% (20/22) of local medical staff in WCEDC participated in the questionnaire survey; 100% (20/20) thought that the BIIS was easy to use while 35% (7/20) thought it was unstable. All medical staff were willing to use it in future works.
HTML
-
This study was the first to evaluate the BIIS. The implementation of BIIS had significantly shortened the delays of brucellosis reporting; made the case diagnosis, treatment, and management more effective; and reduced the workload of data input. It was an effective information connection hub with the HIS and LIS.
The stability of BIIS needs to be further improved. The main reason for the instability of the system was that after the BIIS was connected with the HIS and LIS, the heterogeneous systems were complex and the compatibility was insufficient, which was a problem encountered by most connected hospitals (5-6). It was also necessary to upgrade the integration of the BIIS with HIS and LIS to clearly monitor the process of exchange among the systems (7). Meanwhile, the completeness of BIIS also needs to be improved, which was primarily affected by the lack of epidemiological exposure history of patients. That is, medical staff focused more on diagnosis and treatment according to the clinical symptoms and laboratory results of patients but paid no attention to the epidemiological characteristics. In order to improve the completeness of the system, patient epidemiological history should be set as mandatory check.
This study has subject to some limitations. The BIIS currently only is applied by one hospital in WCEDC. There was needed for more medical institution and for further evaluation of the system.
In summary, the BIIS was evaluated for the first time and demonstrated its advantages and disadvantages, which could provide some evidence for further improvement of the system. The results of the BIIS assessment gave us certain understandings for the future application in other districts in China.
Acknowledgments: Inner Mongolia Center for Comprehensive Disease Control and Prevention and Wulanchabu City Center for Endemic Disease Prevention and Control.
Conflicts of interest: The authors who have taken part in this study declared that they did not have any other potential conflicts of interest.
Funding: National Science and Technology Major Project of China (2018ZX10713001-001).
Ethical Approval and consent to participate: The ethics committee approved the study. Written informed consent has been obtained from the patients in accordance with the Declaration of Helsinki. We confirmed that the identification information of all participants (including patient names, ID numbers, home addresses and telephone numbers) would not be included in recordings, written descriptions or publications.
| Citation: |

|